Post-mortem skeletal surveys in suspected non-accidental injury Y. Hughes-Roberts, O.J. Arthurs, H. Moss, P.A.K. Set * Department of Radiology, Addenbrooke’s Hospital, Cambridge, UK article information Article history: Received 21 December 2011 Received in revised form 15 January 2012 Accepted 25 January 2012 AIM: To evaluate potential differences between live (LSS) and post-mortem skeletal surveys (PMSS) in cases of non-accidental injury (NAI). MATERIALS AND METHODS: All skeletal surveys (SS) performed for suspected NAI over a 5 year period were retrospectively reviewed. Demographic details, injuries obtained, arte- facts, and radiographic difficulties encountered during LSS and PMSS were recorded. RESULTS: Of 195 surveys performed, there were significantly fewer positive PMSS (11/128; 8.6%) than LSS (16/67; 23.8%), but no difference between the actual injuries encountered. Of those who had a positive SS, dead children were significantly younger (mean age 2.6 3.4 months old) than live children (7.8 6.9 months old; p < 0.05). Thirty-six percent of all contemporary digital radiographs contained artefacts, particularly in PMSS (599/1504; 39.8%) compared to LSS (269/904: 29.7%; p < 0.001), which were mostly patient identification labels (55.1 versus 21.6%; p < 0.001). PMSS demonstrated death-related radiographic complications in 10.6% of cases. CONCLUSION: Radiographic imaging in deceased children is not easy, and yields significant artefacts, which may hamper image interpretation. A technique for obtaining multiple views of a limb in fixed flexion deformity to maximize the diagnostic potential is described. Careful consideration of these factors would maximize the diagnostic yield in this unique patient population. Ó 2012 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved. Introduction Complete skeletal surveys (SS) of young infants are reference standard practice in the setting of a suspected non-accidental injury (NAI). A high-detail SS is used to identify known as well as occult fractures, particularly those that may be highly specific for abuse, e.g., the classic met- aphyseal lesion or posterior rib fractures. The specific patterns of bony injury seen in victims of child abuse have been well established and are beyond the scope of this article. 1e4 There are now extensive guidelines on how to perform detailed skeletal radiographs in children suspected of NAI, from British and American faculties, 5e7 although several studies have revealed widespread regional and international variation 8e11 in everyday practice. Unfortunately, the most extreme presentation of NAI is the dead child. Although negative SS do not exclude abuse, they may be useful when combined with other clinical and post-mortem findings, such as in helping to confirm or refute a diagnosis of sudden infant death syndrome (SIDS). There are no specific guidelines or recommendations on how to perform a post-mortem SS (PMSS), or whether full SS are necessary. British guidelines regarding SS for forensic purposes do not comment on the difficulties encountered in post-mortem studies. 12 In fact, the Society for Paediatric Radiology e National Association of Medical Examiners * Guarantor and correspondent: P.A.K. Set, Department of Radiology, Box 219, Addenbrooke’s Hospital, Cambridge University Teaching Hospitals NHS Foundation Trust, Hills Road, Cambridge CB2 0QQ, UK. Tel.: þ44 (0) 1223 216268; fax: þ44 (0) 1223 217847. E-mail address: [email protected](P.A.K. Set). Contents lists available at SciVerse ScienceDirect Clinical Radiology journal homepage: www.clinicalradiologyonline.net 0009-9260/$ e see front matter Ó 2012 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.crad.2012.01.020 Clinical Radiology xxx (2012) 1e9 Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem skeletal surveys in suspected non-accidental injury, Clinical Radiology (2012), doi:10.1016/j.crad.2012.01.020
0009-9260/$ e see front matter � 2012 The Royal Codoi:10.1016/j.crad.2012.01.020
Please cite this article in press as: Hughes-Ro(2012), doi:10.1016/j.crad.2012.01.020
AIM: To evaluate potential differences between live (LSS) and post-mortem skeletal surveys(PMSS) in cases of non-accidental injury (NAI).MATERIALS AND METHODS: All skeletal surveys (SS) performed for suspected NAI over
a 5 year period were retrospectively reviewed. Demographic details, injuries obtained, arte-facts, and radiographic difficulties encountered during LSS and PMSS were recorded.RESULTS: Of 195 surveys performed, there were significantly fewer positive PMSS (11/128;
8.6%) than LSS (16/67; 23.8%), but no difference between the actual injuries encountered. Ofthose who had a positive SS, dead children were significantly younger (mean age 2.6 � 3.4months old) than live children (7.8 � 6.9 months old; p < 0.05). Thirty-six percent of allcontemporary digital radiographs contained artefacts, particularly in PMSS (599/1504; 39.8%)compared to LSS (269/904: 29.7%; p < 0.001), which were mostly patient identification labels(55.1 versus 21.6%; p < 0.001). PMSS demonstrated death-related radiographic complicationsin 10.6% of cases.CONCLUSION: Radiographic imaging in deceased children is not easy, and yields significant
artefacts, which may hamper image interpretation. A technique for obtaining multiple views ofa limb in fixed flexion deformity to maximize the diagnostic potential is described. Carefulconsideration of these factors would maximize the diagnostic yield in this unique patientpopulation.
� 2012 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Introduction
Complete skeletal surveys (SS) of young infants arereference standard practice in the setting of a suspectednon-accidental injury (NAI). A high-detail SS is used toidentify known as well as occult fractures, particularly thosethat may be highly specific for abuse, e.g., the classic met-aphyseal lesion or posterior rib fractures. The specificpatterns of bony injury seen in victims of child abuse havebeen well established and are beyond the scope of this
epartment of Radiology,iversity Teaching HospitalsB2 0QQ, UK. Tel.: þ44 (0)
.A.K. Set).
llege of Radiologists. Published by
berts Y, et al., Post-mortem s
article.1e4 There are now extensive guidelines on how toperform detailed skeletal radiographs in children suspectedof NAI, from British and American faculties,5e7 althoughseveral studies have revealed widespread regional andinternational variation8e11 in everyday practice.
Unfortunately, the most extreme presentation of NAI isthe dead child. Although negative SS do not exclude abuse,they may be useful when combined with other clinical andpost-mortem findings, such as in helping to confirm orrefute a diagnosis of sudden infant death syndrome (SIDS).There are no specific guidelines or recommendations onhow to perform a post-mortem SS (PMSS), or whether fullSS are necessary. British guidelines regarding SS for forensicpurposes do not comment on the difficulties encountered inpost-mortem studies.12 In fact, the Society for PaediatricRadiology e National Association of Medical Examiners
Elsevier Ltd. All rights reserved.
keletal surveys in suspected non-accidental injury, Clinical Radiology
Y. Hughes-Roberts et al. / Clinical Radiology xxx (2012) 1e92
(SPR-NAME) guidance paper suggested that the full 20 or soradiographs obtained in a live child are rarely necessary indeceased children because during the autopsy a pathologistcan directly examine the axial skeleton,13 suggesting thatwell-collimated views of the long bones could suffice.Several studies havemore recently demonstrated that PMSScan identify skeletal injuries, including metaphyseal frac-tures, which were not detected at routine autopsy.14e16
PMSS can also provide additional information about theextent and chronicity of extremity trauma that would notbe detected by routine post-mortem, and additional infor-mation such as stages of bone maturation.17
The present authors have performed full SS in both liveand deceased children for more than 10 years, and a signifi-cant proportion of the authors’workload consists of imagingdeceased children, as Addenbrooke’s Hospital is the regionalcentre for peri-natal and paediatric post-mortem studies.The aim of this study was to evaluate and quantify thepotential differences between live SS, LSS, PMSS withparticular attention to demography, differences in theinjuries encountered, and radiographic difficulties.
Table 1Minimum skeletal survey radiographs performed at Addenbrooke’s Hospital,irrespective of whether the child is live or deceased.
Body part Radiographs Description
Head 3 Skull anteroposterior, lateral andTowne’s view
Thorax 3 Anteroposterior chest including neck,left andright oblique views of the ribs
Abdomen 1 Single anteroposterior abdomenincluding pelvis
Spine 1 Single lateral thoraco-lumbar spineincluding neck
Limbs 4 Left and right anteroposterior &lateral knee
4 Left and right anteroposterior &lateral elbow
4 Left and right anteroposterior &lateral ankle
4 Left and right Dorsipalmar & lateral wristHands 2 Dorsipalmar handsFeet 2 Dorsiplantar feetTOTAL 28
The surveys contain more than the current recommendations as limb radio-graphs are centred on joints (e.g., elbow) instead of bones (e.g., radius) so thatareas suchasmetaphyses arewithin the centre of the radiographicfield. Conedviews or views of the lateral cervical spine are added in individual cases.
Materials and methods
All SS performed on children for suspected NAI performedat Addenbrooke’s Hospital over a 5 year period (2005e2009),which were performed on children below the age of 5 years,were retrospectively reviewed. Ethical approval was notrequired for this retrospective study, according to local ethicalcommittee guidance. Standard demographic details wererecorded for each child, including age, gender, positiveradiographic findings; the presence and nature of radio-graphic artefacts, and any difficulties encountered inacquiring adequate radiographic images, such as rigormortis.
SS were performed prior to autopsy in all cases, althoughthe final cause of death was not recorded. SS were consid-ered positive if a single injury or multiple injuries werepresent with a high index of suspicion of NAI. In the PMgroup, all coroner’s caseswere included, including suspicious(possible SIDS) and non-suspicious deaths where a full SSwas performed, in order to create the best comparativegroup to the full LSS group. Many foetuses or terminations ofpregnancy, and neonatal deaths in whom a limited “baby-gram” or incomplete survey was performed, were excludedin order to provide as close a comparison between live andPM cases. All examinations were performed in the radiologydepartment in order to retain consistency. PMSS were per-formed in the Department of Radiology in the presence ofa paediatric biomedical scientist, rather than the mortuary,in order to provide the best possible imaging using staticrather than mobile machines, and best possible comparisonbetween the two groups.
First, all SS were reviewed for the presence or absence ofsignificant injuries, together with the original radiologyreport. This included several packets of plain radiographs,as well as more recent digital radiographs stored on thepicture archiving and communication system (PACS). Inorder to exclude artefacts generated through plain film
Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem s(2012), doi:10.1016/j.crad.2012.01.020
storage, and to provide contemporary informationregarding artefacts, only those SS that were present on thePACS system were included for detailed artefact analysis.
The local SS protocol was established over 15 years ago(Table 1), includes 28 images per examination, and is per-formed by two named, dedicated paediatric radiographers ineach case, irrespective of whether the child imaged is alive ordeceased. The protocol includes more views than thoserecommended in the 2008 Royal College of Paediatrics andChild Health (RCPCH)/Royal College of Radiologists (RCR)guidelines,6 mainly because a greater number of limb viewsare included, centred on the joints rather than long bones, toallow for careful interrogation of the metaphyseal regions.
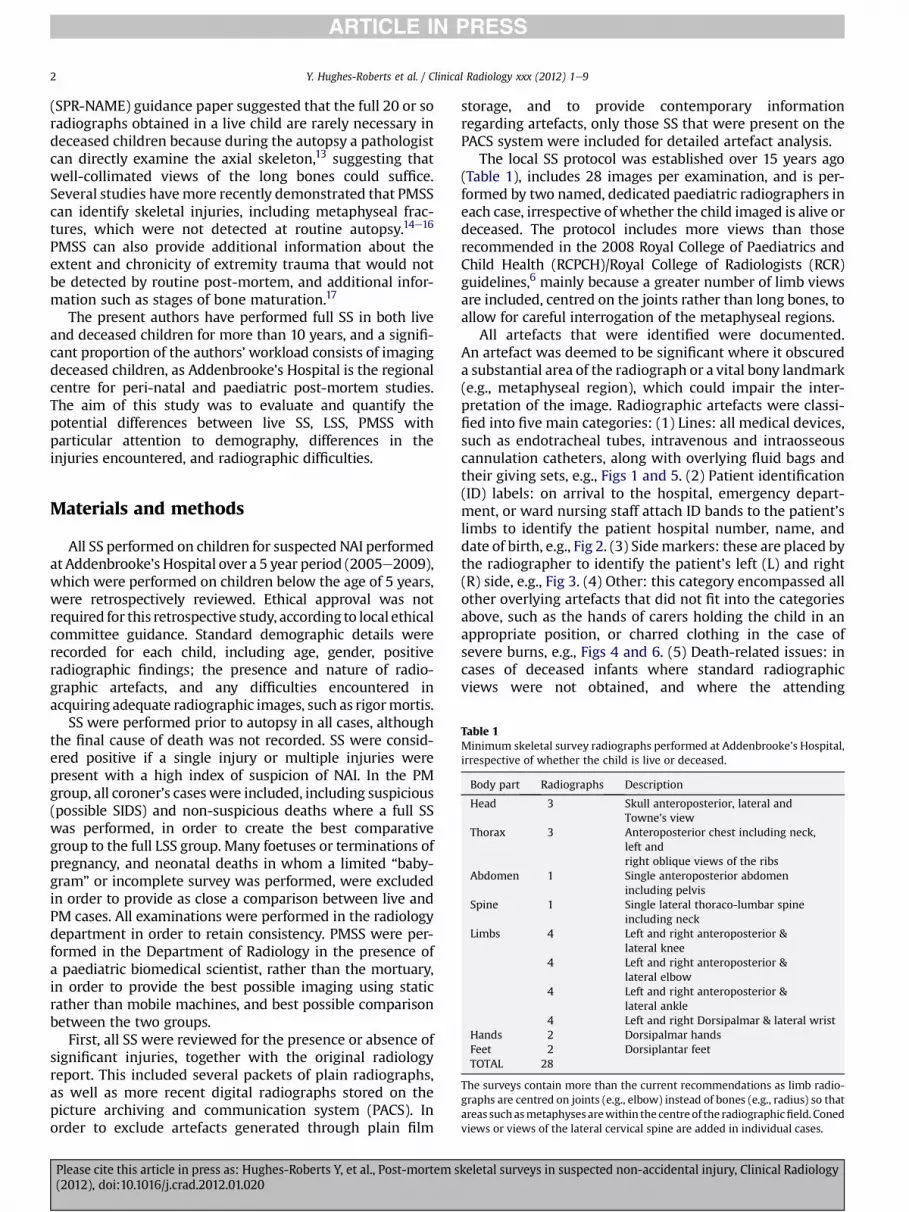
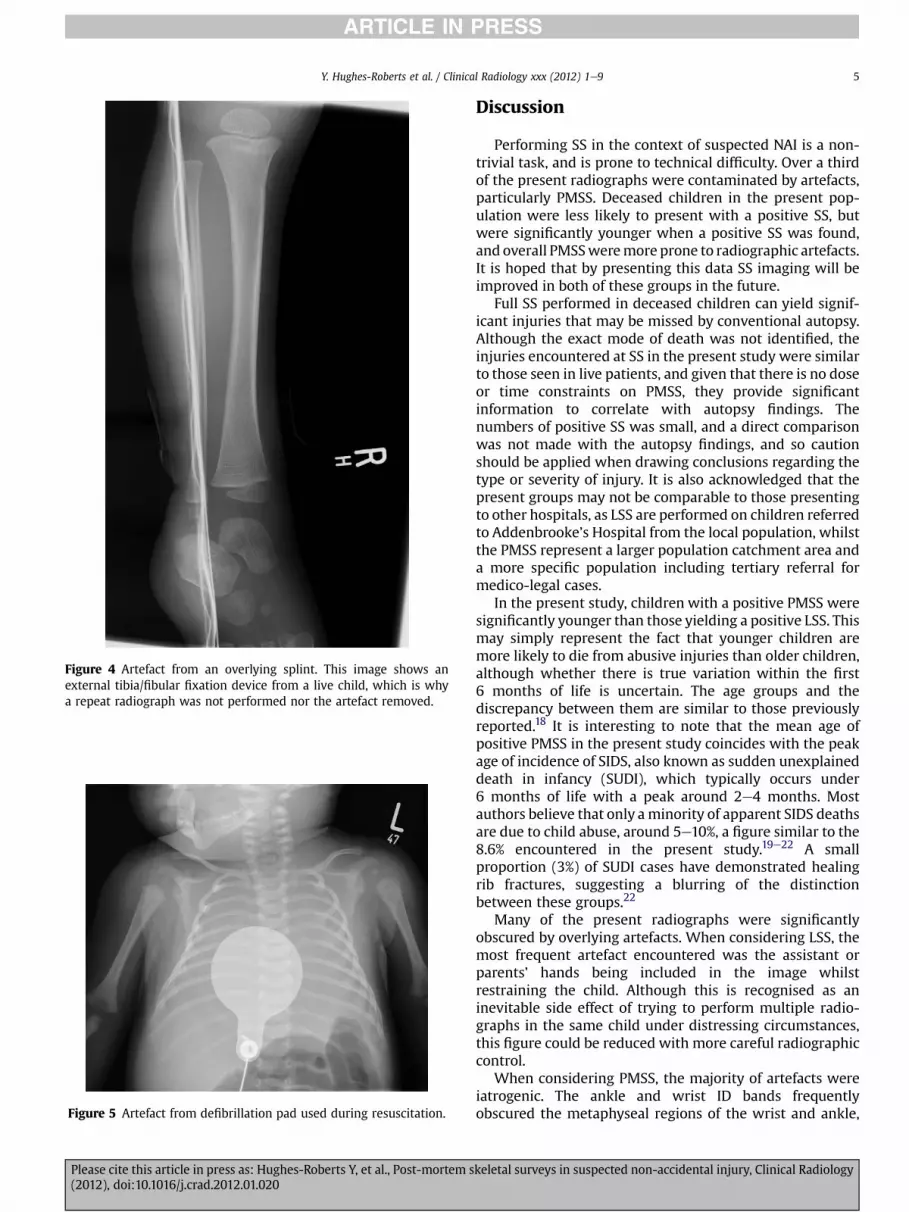
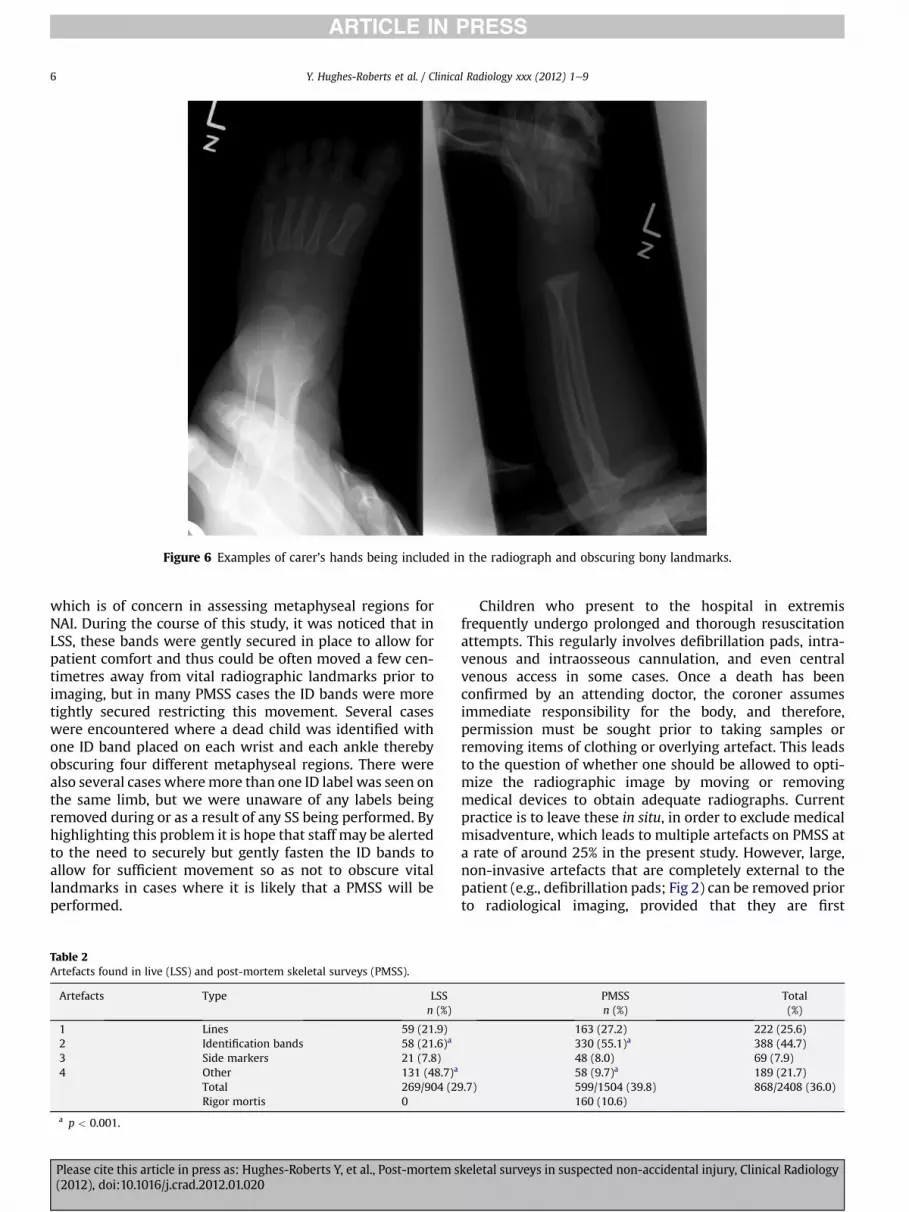
All artefacts that were identified were documented.An artefact was deemed to be significant where it obscureda substantial area of the radiograph or a vital bony landmark(e.g., metaphyseal region), which could impair the inter-pretation of the image. Radiographic artefacts were classi-fied into five main categories: (1) Lines: all medical devices,such as endotracheal tubes, intravenous and intraosseouscannulation catheters, along with overlying fluid bags andtheir giving sets, e.g., Figs 1 and 5. (2) Patient identification(ID) labels: on arrival to the hospital, emergency depart-ment, or ward nursing staff attach ID bands to the patient’slimbs to identify the patient hospital number, name, anddate of birth, e.g., Fig 2. (3) Sidemarkers: these are placed bythe radiographer to identify the patient’s left (L) and right(R) side, e.g., Fig 3. (4) Other: this category encompassed allother overlying artefacts that did not fit into the categoriesabove, such as the hands of carers holding the child in anappropriate position, or charred clothing in the case ofsevere burns, e.g., Figs 4 and 6. (5) Death-related issues: incases of deceased infants where standard radiographicviews were not obtained, and where the attending
keletal surveys in suspected non-accidental injury, Clinical Radiology
Figure 1 Intravenous cannula and intraosseous needles, with the associated fixation devices, can cause artefacts.
Figure 2 Patient identification labels are typically placed on the wrist of the patient on arrival in the hospital, but can obscure metaphysealregions.
Y. Hughes-Roberts et al. / Clinical Radiology xxx (2012) 1e9 3
Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem skeletal surveys in suspected non-accidental injury, Clinical Radiology(2012), doi:10.1016/j.crad.2012.01.020
Figure 3 Examples of artefacts: radiographic side markers are used to denote the left or right of the patient, but can obscure important bonylandmarks.
Y. Hughes-Roberts et al. / Clinical Radiology xxx (2012) 1e94
radiographer had documented that the child suffered fixedflexion deformity, typically of the hands, feet, elbows, andknees, e.g., Fig 8.
Statistical analysis was performed using Student’s t-testfor continuous, normally distributed data (e.g., age) andusing Chi-squared testing between the two groups usingSPSS 18.0 for Windows (SPSS, Chicago, IL, USA) at the 5%level of significance.
Results
One hundred and ninety nine SS were performed forsuspected NAI over a 5 year period. Four examinations wereexcluded; three were not available for analysis, and in onecase a diagnosis of skeletal dysplasia was made, thusyielding 195 complete SS for suspected NAI for review.
Demographics
The mean age of all cases was 7.1 � 9.2 months (range2 days to 4.5 years) with 188/195 under the age of 2 years,and 29 of the total 195 SS were abnormal (14.8%). Onehundred and ninety-five cases yielded 67 LSS (34.3%) and128 (65.6%) PMSS. There was no statistical differencebetween the ages (LSS: 6.8 � 6.6 months old; PMSS: age7.2 � 10.2 months old; p ¼ ns) or genders of the two groups(LSS: 59% male; PMSS: 63% male; p ¼ ns).
Injuries encountered
There were statistically more abnormal LSS than PMSS;16/67 LSS were identified as abnormal (23.8%), whichincluded six skull fractures, nine long bone fractures, andfour cases of multiple injuries. Eleven of 128 the PMSS
Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem s(2012), doi:10.1016/j.crad.2012.01.020
studies (8.6%; p < 0.05) were abnormal, including five skullfractures, four long bone fractures, and five multiple frac-tures. Multiple fractures usually included ribs, long bones,and metaphyseal regions. There were no significant statis-tical differences between the incidence of individual skull,long bone, or multiple fractures between the two groups. Ofthose who had a positive SS, the 11 PMSS were significantlyyounger (mean age 2.6� 3.4months old) than LSS (7.8� 6.9months old; p < 0.05). No child had a LSS and subsequentlydied of their injuries.
Artefacts
The most recent 99 SS on PACS were available for detailedartefact assessment, yielding a total of 2408 radiographs.Eight hundred and sixty-eight radiographs (36%) containedartefacts, of which the majority (566/868; 65.2%) werejudged to be significant. There were significantly moreartefacts on radiographs performed in PMSS (599/1504;39.8%) compared to LSS (269/904: 29.7%; p < 0.001), andmore artefacts were judged to be significant in PMSS (426/599: 71%) compared to LSS (140/269: 53%; p < 0.001).
Overall, the majority of artefacts were iatrogenic: eitherpatient ID markers (44.7%) or medically placed lines anddevices (25.6%; Figs 1e6). A full description of the types ofartefacts encountered is given in Table 2: there weresignificantly more patient ID artefacts in PMSS (55.1 versus21.6%; p < 0.001) but significantly more “other” artefacts inLSS (48.7 versus 9.7%: p < 0.001).
One hundred and sixty out of 1504 (10.6%) PMSS radio-graphs demonstrated rigormortis artefact as a complicationof death, typically manifest as fixed flexion deformities ofthe hands/fingers and knees (e.g., Fig 7).
keletal surveys in suspected non-accidental injury, Clinical Radiology
Figure 4 Artefact from an overlying splint. This image shows anexternal tibia/fibular fixation device from a live child, which is whya repeat radiograph was not performed nor the artefact removed.
Figure 5 Artefact from defibrillation pad used during resuscitation.
Y. Hughes-Roberts et al. / Clinical Radiology xxx (2012) 1e9 5
Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem s(2012), doi:10.1016/j.crad.2012.01.020
Discussion
Performing SS in the context of suspected NAI is a non-trivial task, and is prone to technical difficulty. Over a thirdof the present radiographs were contaminated by artefacts,particularly PMSS. Deceased children in the present pop-ulation were less likely to present with a positive SS, butwere significantly younger when a positive SS was found,and overall PMSSweremore prone to radiographic artefacts.It is hoped that by presenting this data SS imaging will beimproved in both of these groups in the future.
Full SS performed in deceased children can yield signif-icant injuries that may be missed by conventional autopsy.Although the exact mode of death was not identified, theinjuries encountered at SS in the present study were similarto those seen in live patients, and given that there is no doseor time constraints on PMSS, they provide significantinformation to correlate with autopsy findings. Thenumbers of positive SS was small, and a direct comparisonwas not made with the autopsy findings, and so cautionshould be applied when drawing conclusions regarding thetype or severity of injury. It is also acknowledged that thepresent groups may not be comparable to those presentingto other hospitals, as LSS are performed on children referredto Addenbrooke’s Hospital from the local population, whilstthe PMSS represent a larger population catchment area anda more specific population including tertiary referral formedico-legal cases.
In the present study, children with a positive PMSS weresignificantly younger than those yielding a positive LSS. Thismay simply represent the fact that younger children aremore likely to die from abusive injuries than older children,although whether there is true variation within the first6 months of life is uncertain. The age groups and thediscrepancy between them are similar to those previouslyreported.18 It is interesting to note that the mean age ofpositive PMSS in the present study coincides with the peakage of incidence of SIDS, also known as sudden unexplaineddeath in infancy (SUDI), which typically occurs under6 months of life with a peak around 2e4 months. Mostauthors believe that only aminority of apparent SIDS deathsare due to child abuse, around 5e10%, a figure similar to the8.6% encountered in the present study.19e22 A smallproportion (3%) of SUDI cases have demonstrated healingrib fractures, suggesting a blurring of the distinctionbetween these groups.22
Many of the present radiographs were significantlyobscured by overlying artefacts. When considering LSS, themost frequent artefact encountered was the assistant orparents’ hands being included in the image whilstrestraining the child. Although this is recognised as aninevitable side effect of trying to perform multiple radio-graphs in the same child under distressing circumstances,this figure could be reduced with more careful radiographiccontrol.
When considering PMSS, the majority of artefacts wereiatrogenic. The ankle and wrist ID bands frequentlyobscured the metaphyseal regions of the wrist and ankle,
keletal surveys in suspected non-accidental injury, Clinical Radiology
Figure 6 Examples of carer’s hands being included in the radiograph and obscuring bony landmarks.
Y. Hughes-Roberts et al. / Clinical Radiology xxx (2012) 1e96
which is of concern in assessing metaphyseal regions forNAI. During the course of this study, it was noticed that inLSS, these bands were gently secured in place to allow forpatient comfort and thus could be often moved a few cen-timetres away from vital radiographic landmarks prior toimaging, but in many PMSS cases the ID bands were moretightly secured restricting this movement. Several caseswere encountered where a dead child was identified withone ID band placed on each wrist and each ankle therebyobscuring four different metaphyseal regions. There werealso several cases wheremore than one ID label was seen onthe same limb, but we were unaware of any labels beingremoved during or as a result of any SS being performed. Byhighlighting this problem it is hope that staff may be alertedto the need to securely but gently fasten the ID bands toallow for sufficient movement so as not to obscure vitallandmarks in cases where it is likely that a PMSS will beperformed.
Table 2Artefacts found in live (LSS) and post-mortem skeletal surveys (PMSS).
Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem s(2012), doi:10.1016/j.crad.2012.01.020
Children who present to the hospital in extremisfrequently undergo prolonged and thorough resuscitationattempts. This regularly involves defibrillation pads, intra-venous and intraosseous cannulation, and even centralvenous access in some cases. Once a death has beenconfirmed by an attending doctor, the coroner assumesimmediate responsibility for the body, and therefore,permission must be sought prior to taking samples orremoving items of clothing or overlying artefact. This leadsto the question of whether one should be allowed to opti-mize the radiographic image by moving or removingmedical devices to obtain adequate radiographs. Currentpractice is to leave these in situ, in order to exclude medicalmisadventure, which leads to multiple artefacts on PMSS ata rate of around 25% in the present study. However, large,non-invasive artefacts that are completely external to thepatient (e.g., defibrillation pads; Fig 2) can be removed priorto radiological imaging, provided that they are first
keletal surveys in suspected non-accidental injury, Clinical Radiology
Figure 8 Imaging above the joint. By aiming the beam towards thefemur, the distal femur becomes more apparent.
Figure 7 Conventional anteroposterior and lateral views of the knee during PMSS. Whilst the lateral view is good, the conventionalanteroposterior view of the knee projects both the femur and tibia at an oblique plane due to the fixed flexion deformity.
Y. Hughes-Roberts et al. / Clinical Radiology xxx (2012) 1e9 7
photographed in situ. Also, the external components ofinternal devices (e.g., the part of an endotracheal tube,which protrudes from the mouth, or the tubing attached toan intravenous device) can be removed or cut, as they arealso external to the patient. However, all tubes and linesthat are internal or attached to the patient cannot beremoved before PM, unless there is explicit permissionsought and gained from the coroner’s office. No permissionsof this kind were sought during the course of the study, butmore careful placement of potential artefacts in the future,may be the more considerate approach. Although theinsertion of cannulas during resuscitation cannot be influ-enced by potential prospective conflicts at PMSS, theplacement and number of patient ID bands can be adjustedso as to minimize disruption to a future PMSS.
Rigor mortis refers to the state of the body after death, inwhich muscles stiffen. The process begins 3 h after death,reaching maximum stiffness within 12 h and then graduallydissipating until around 72 h after death. It occurs due tochanges in muscle physiology when aerobic respirationceases: cessation of ionic flux results in increased intracel-lular calcium concentrations, which causes musclecontraction. Unfortunately, the timing of rigor mortiscoincides with optimal timing of a PMSS, between 12 and48 h after death. The implication for PMSS is that musclecontraction may prohibit accurate frontal images of allrequired bones and joints, which was true in 10% of thepresent PMSS cases. Recent guidelines state that: “The limbsmust be straight”,6 but this proved particularly difficult atthe elbows, knees, and hands when encountered in a fixedflexion deformity. One suggestion to overcome this, whichthe present authors have used for over 3 years, is to performthree anteroposterior views as well as the lateral view of
Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem s(2012), doi:10.1016/j.crad.2012.01.020
limbs in fixed flexion. For instance, at the knee joint, sepa-rate radiographs are performed centring on the joint (knee;Fig 7), centring on the bone above (femur; Fig 8), and thebone below the joint (tibia; Fig 9).
keletal surveys in suspected non-accidental injury, Clinical Radiology
Figure 9 Imaging below the joint. By aiming the beam towards thetibia, the proximal tibia becomes more apparent.
Y. Hughes-Roberts et al. / Clinical Radiology xxx (2012) 1e98
Some authors believe that PMSS are not necessary andthat a formal PM will suffice; however, several studies havereported skeletal injuries detected by radiographs that weremissed on conventional PM examinations.14e16 Althoughcross-sectional imaging including computed tomography(CT) and magnetic resonance imaging (MRI) are becomingincreasingly used in PM work, with increasing interest inminimally invasive autopsy, standard skeletal radiographswill continue to play a key role in providing complimentaryinformation to conventional autopsy in future.23
Limitations of this study
One of the limitations of all retrospective studies is thepopulation sample, which in the present study may not berepresentative of the experience of other centres. However,the artefacts encountered probably represent typicalwestern medical care and are likely to be encountered inthis scenario in other hospitals.
The focus of the present study was SS, so other forms ofcross-sectional imaging were not reviewed (e.g., headimaging) nor what the outcome was. A higher incidence offatal brain injury in one group is a possible explanation ofthe differences observed, as this is a common cause of deathin the suspected NAI population.
Less than 10% of the present radiographs were obscuredby a left/right side marker, but the number of occasions inwhich the marker was not placed on the radiograph at allwas not counted, which would be considered by some to bea bigger problem. Indeed, to this extent, the RCR and Society& College of Radiographers (SCoR) have issued recentguidelines discussing whether radiographs should berepeated in the case of a side marker being inadvertently
Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem s(2012), doi:10.1016/j.crad.2012.01.020
obscured or not present.24 Whilst it is easy to re-acquireradiographs during PMSS, it would depend on the errorbeing identified in a timely fashion, but clearly poses a moresignificant problem during LSS.
Not all hospitals will be able to provided dedicatedexperienced paediatric radiographers to perform all SS,despite recommendations to this extent. In the presentstudy, PMSSs are performed by a small group of fourexperienced radiographers, led by one senior radiographerwho has had forensic training. (Further information can beobtained from the International Association of ForensicRadiographers (http://www.afr.org.uk/)) Whilst these arestrengths of the present study, the number of artefactsdescribed here could be interpreted as a “best case”scenario from an experienced team, which may be expectedto be worse in other departments.
In conclusion, performing SS in children is not easy, andyields significant artefacts, which may hamper imageinterpretation. PMSS can reveal significant bony abnor-malities similar to those encountered in LSS. PMSS areprone to iatrogenic radiographic artefacts following resus-citation or difficulties in obtaining traditional views due torigor mortis, and one technique is described for obtainingmultiple views of a limb in fixed flexion deformity. Carefulconsideration of all of these factors in the future wouldmaximize the diagnostic yield in this unique patientpopulation.
Acknowledgements
The authors acknowledge the assistance of Nikki Hall,Paediatric Mortuary Services Manager in Cambridge, forassistance in preparation of the manuscript.
References
1. Kleinman PK, Marks SC, Blackbourne B. The metaphyseal lesion inabused infants: a radiologicehistopathologic study. AJR Am J Roentgenol1986;146:895e905.
2. Kleinman PK, Marks Jr SC, Richmond JM, et al. Inflicted skeletal injury:a postmortem radiologicehistopathologic study in 31 infants. AJR AmJ Roentgenol 1995;165:647e50.
3. Kogutt MS, Swischuk LE, Fagan CJ. Patterns of injury and significance ofuncommon fractures in the battered child syndrome. AJR Am J Roent-genol 1974;121:143e9.
4. Kemp AM, Dunstan F, Harrison S, et al. Patterns of skeletal fractures inchild abuse: systematic review. BMJ 2008;337:a1518.
5. British Society of Paediatric Radiology. Standard for skeletal surveys insuspected non-accidental injury (NAI) in children, http://www.bspr.org.uk/nai.htm; 2008 [accessed October 2011].
6. The Royal College of Child Health and Paediatrics and The Royal Collegeof Radiologists. Standards for radiological investigations of suspected non-accidental injury. London: RCPCH; 2008. ref.: BFCR(08)1.
7. ACR guidelines. ACR practice guidelines for skeletal surveys in children.revised 2001 and 2006. American College of Radiology, USA; 1997[accessed October 2011].
8. Offiah AC, Hall CM. Observational study of skeletal surveys in suspectednon-accidental injury. Clin Radiol 2003;58:702e5.
9. James SL, Halliday K, Somers J, et al. A survey of non-accidental injuryimaging in England, Scotland and Wales. Clin Radiol 2003;58:696e701.
10. Swinson S, Tapp M, Brindley R, et al. An audit of skeletal surveys forsuspected non-accidental injury following publication of the BritishSociety of Paediatric Radiology guidelines. Clin Radiol 2008;63:651e6.
keletal surveys in suspected non-accidental injury, Clinical Radiology
12. The Society and College of Radiographers. Skeletal survey for suspectedNAI, SIDS and SUDI: guidance for radiographers, http://doc-lib.sor.org/skeletal-survey-suspected-non-accidental-injury; 2009 [accessedOctober 2011].
13. Mendleson KL. The Society for Pediatric Radiology e National Associa-tion of Medical Examiners. Post-mortem radiography in the evaluationof unexpected death in children less than 2 years of age whose death issuspicious for fatal abuse. Pediatr Radiol 2004;34:675e7.
14. Kremer C, Racette S, Marton D, et al. Radiographs interpretation by forensicpathologists: a word of warning. Am J Forensic Med Pathol 2008;29:295e6.
15. Kleinman PK, Blackbourne BD, Marks SC, et al. Radiologic contributionsto the investigation and prosecution of cases of fatal infant abuse. N EnglJ Med 1989;320:507e11.
16. McGraw EP, Pless JE, Pennington DJ, et al. Postmortem radiography afterunexpected death in neonates, infants and children: should imaging beroutine? AJR Am J Roentgenol 2002;178:1517e21.
17. Olsen RE. Radiography following perinatal death: a review. Acta Radiol2006;47:91e9.
Please cite this article in press as: Hughes-Roberts Y, et al., Post-mortem s(2012), doi:10.1016/j.crad.2012.01.020
18. De Lange C, Vege A, Stake G. Radiography after unexpected death ininfants and children compared to autopsy. Pediatr Radiol2007;37:159e65.
19. Emery JL. Child abuse, sudden infant death syndrome, and unexpectedinfant death. Am J Dis Child 1993;147:1097e100.
20. Distinguishing Sudden Infant Death Syndrome from Child AbuseFatalities. Committee on child abuse and neglect. Pediatrics1994;94:124e6.
21. Thomsen TK, Elle B, Thomsen JL. Post-mortem radiological examinationin infants: evidence of child abuse? Forensic Sci Int 1997;90:223e30.
22. Weber MA, Risdon RA, Offiah AC, et al. Rib fractures identified at post-mortem examination in sudden unexpected deaths in infancy (SUDI).Forensic Sci Int 2009;189:75e81.
23. Thayyil S, Chitty LS, Robertson NJ, et al. Minimally invasive fetal post-mortem examination using magnetic resonance imaging and compu-terised tomography: current evidence and practical issues. Prenat Diagn2010;30:713e8.
24. The Royal College of Radiologists and The Society and College of Radi-ographers. Imaging for non-accidental injury, use of anatomicalmarkers. BFCR(5), http://rcr.ac.uk/docs/radiology/pdf/BFCR(11)5_RCR_COR_NAI.pdf, 2011;11 [accessed October 2011].
keletal surveys in suspected non-accidental injury, Clinical Radiology