CASE REPORT Suspected clindamycin-associated oesophageal injury in cats: five cases Julia A Beatty BSc(hons), BVetMed, PhD, FACVSc (Feline Medicine), MRCVS 1 *, Nigel Swift BVetMed, Dip ACVIM (Small Animal Internal Medicine), MRCVS 2 , Darren J Foster BSc, BVMS, PhD, FACVSc (Feline Medicine) 3 , Vanessa RD Barrs BVSc(hons), MVetClinStud, FACVSc (Feline Medicine) 1 1 Valentine Charlton Cat Centre, Faculty of Veterinary Science, University of Sydney, NSW 2006, Australia 2 Animal Referral Hospital, 444 Liverpool Road, South Strathfield, NSW 2136, Australia 3 Veterinary Specialist Centre, PO Box 307, North Ryde, NSW 2113, Australia The clinical findings, treatment and outcome of suspected clindamycin-associated oesophageal injury in five cats are reported. All cats were treated with one 75 mg clindamycin capsule twice daily (dose range 12e19 mg/kg). Capsules were administered without food or a water bolus. Dysphagia, regurgitation, choking or gagging were seen 3e9 days after starting clindamycin. On oesophagoscopy, three cats had oesophagitis, one of which progressed to stricture formation. Two cats had an oesophageal stricture at first presentation. This is the first report of suspected clindamycin-associated oesophageal injury in cats. It serves to further alert practitioners to the potential for drug-induced oesophageal disorders (DIOD) in cats treated with oral medications and to urge prevention by promoting a change in dosing practices. Date accepted: 24 April 2006 Ó 2006 ESFM and AAFP. Published by Elsevier Ltd. All rights reserved. D rug-induced oesophageal disorders (DIOD) are a common clinical diagnosis in humans with normal oesophageal function (Boyce 1998). Over 70 medications have been implicated and more than half of all cases are caused by antibiotics (Levine 1999). Improper ingestion promoting prolonged oesophageal re- tention is crucial in the pathogenesis (Kirkendall 1999). Severe oesophageal damage resulting in stricture formation has been associated with the administration of doxycycline hydrochloride by dry swallow to cats (Melendez et al 2000, Leib et al 2001, McGrotty and Knottenbelt 2002, German et al 2005). We report the clinical findings, treatment and outcome of five cases of suspected clindamy- cin-associated oesophageal injury in cats. Case reports Case 1 An 8-year-old female neutered Birman cat was presented with a 2-week history of regurgitation and weight loss. Seventeen days prior to presentation, the cat had been treated for chronic, intermittent bilateral nasal discharge with clinda- mycin hydrochloride capsules (Antirobe; Pfizer) (17 mg/kg per os every 12 h). After 3 days of treat- ment, the cat was noted by the owner, a veterinary student, to regurgitate during eating. Treatment was stopped but the cat continued to regurgitate and was presented to the Valentine Charlton Cat Centre (VCCC). No major abnormalities were de- tected on physical examination, routine haematol- ogy, serum biochemistry or thoracic radiographs. On oesophagoscopy, an area of circumferential, oesophageal ulceration was observed 3e5 cm dis- tal to the proximal oesophageal sphincter (Fig 1). The cat was treated with parenteral prednisolone sodium succinate (Solu Delta Cortef; Pharmacia) (1 mg/kg subcutaneously every 24 h) amoxycilline clavulanate (Clavulox; Pfizer) (14 mg/kg SC every 12 h), omeprazole (Losec; Astra Zeneca) 1 mg/kg intravenously over 1 h every 24 h) for 2 days and sucralfate suspension (Carafate; Aspen Pharmacare) (250 mg PO every 12 h 7 days). Solids were withheld for 24 h and intravenous *Corresponding author. E-mail: [email protected]Journal of Feline Medicine and Surgery (2006) 8, 412e419 doi:10.1016/j.jfms.2006.04.006 1098-612X/06/060412+08 $32.00/0 Ó 2006 ESFM and AAFP. Published by Elsevier Ltd. All rights reserved. at University of Sydney on May 22, 2013 jfm.sagepub.com Downloaded from
Transcript
CASE REPORT
Suspected clindamycin-associated oesophagealinjury in cats: five cases
Julia A Beatty BSc(hons), BVetMed, PhD, FACVSc (Feline Medicine), MRCVS1*,
Nigel Swift BVetMed, Dip ACVIM (Small Animal Internal Medicine), MRCVS2,
Darren J Foster BSc, BVMS, PhD, FACVSc (Feline Medicine)3,
1Valentine Charlton Cat Centre,Faculty of Veterinary Science,University of Sydney, NSW 2006,Australia2Animal Referral Hospital, 444Liverpool Road, South Strathfield,NSW 2136, Australia3Veterinary Specialist Centre, POBox 307, North Ryde, NSW 2113,Australia
The clinical findings, treatment and outcome of suspectedclindamycin-associated oesophageal injury in five cats are reported. All catswere treated with one 75 mg clindamycin capsule twice daily (dose range12e19 mg/kg). Capsules were administered without food or a water bolus.Dysphagia, regurgitation, choking or gagging were seen 3e9 days after startingclindamycin. On oesophagoscopy, three cats had oesophagitis, one of whichprogressed to stricture formation. Two cats had an oesophageal stricture at firstpresentation. This is the first report of suspected clindamycin-associatedoesophageal injury in cats. It serves to further alert practitioners to the potentialfor drug-induced oesophageal disorders (DIOD) in cats treated with oralmedications and to urge prevention by promoting a change in dosing practices.
Date accepted: 24 April 2006 ! 2006 ESFM and AAFP. Published by Elsevier Ltd. All rights reserved.
D rug-induced oesophageal disorders(DIOD) are a common clinical diagnosisin humans with normal oesophageal
function (Boyce 1998). Over 70 medications havebeen implicated and more than half of all casesare caused by antibiotics (Levine 1999). Improperingestion promoting prolonged oesophageal re-tention is crucial in the pathogenesis (Kirkendall1999). Severe oesophageal damage resulting instricture formation has been associated with theadministration of doxycycline hydrochloride bydry swallow to cats (Melendez et al 2000, Leib et al2001, McGrotty and Knottenbelt 2002, German et al2005). We report the clinical findings, treatmentand outcome of five cases of suspected clindamy-cin-associated oesophageal injury in cats.
Case reports
Case 1
An 8-year-old female neutered Birman cat waspresented with a 2-week history of regurgitation
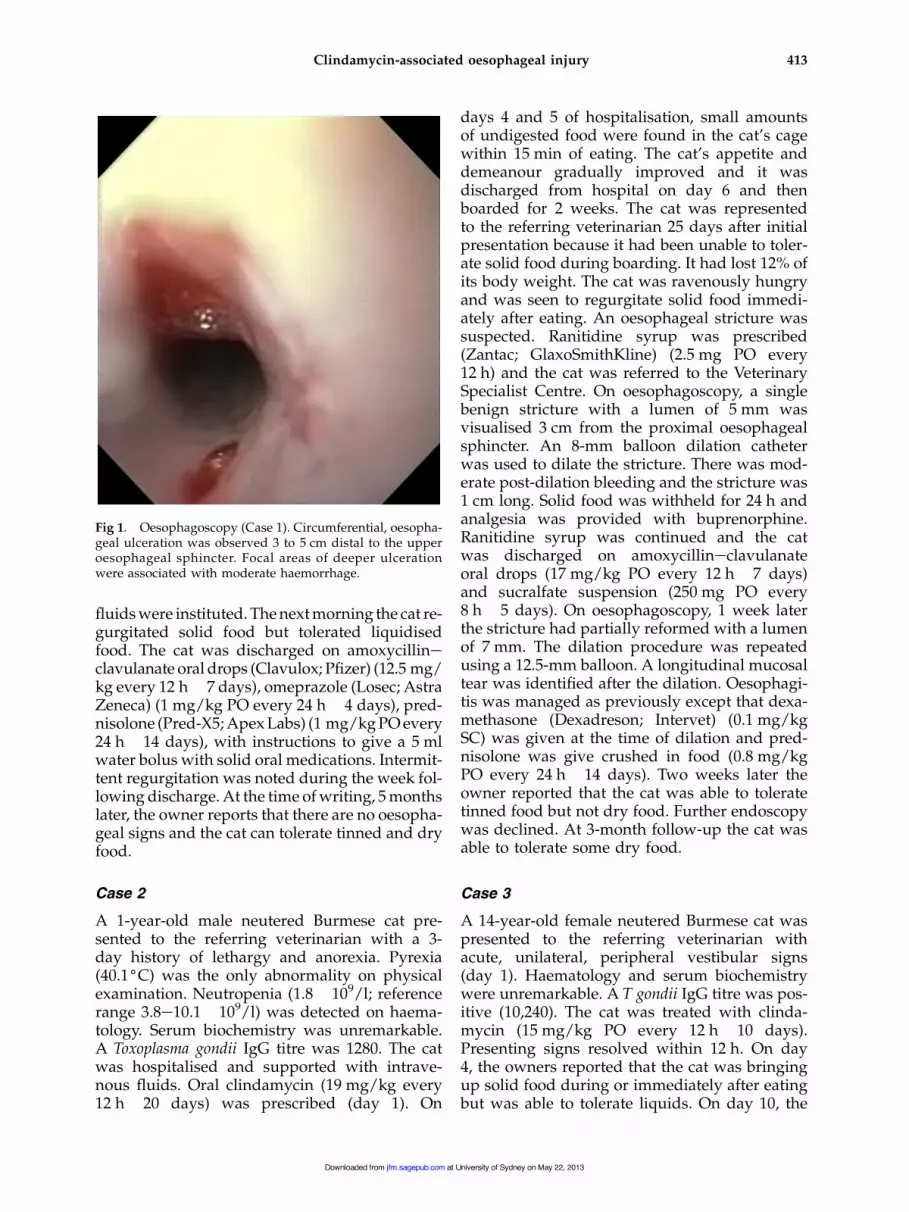
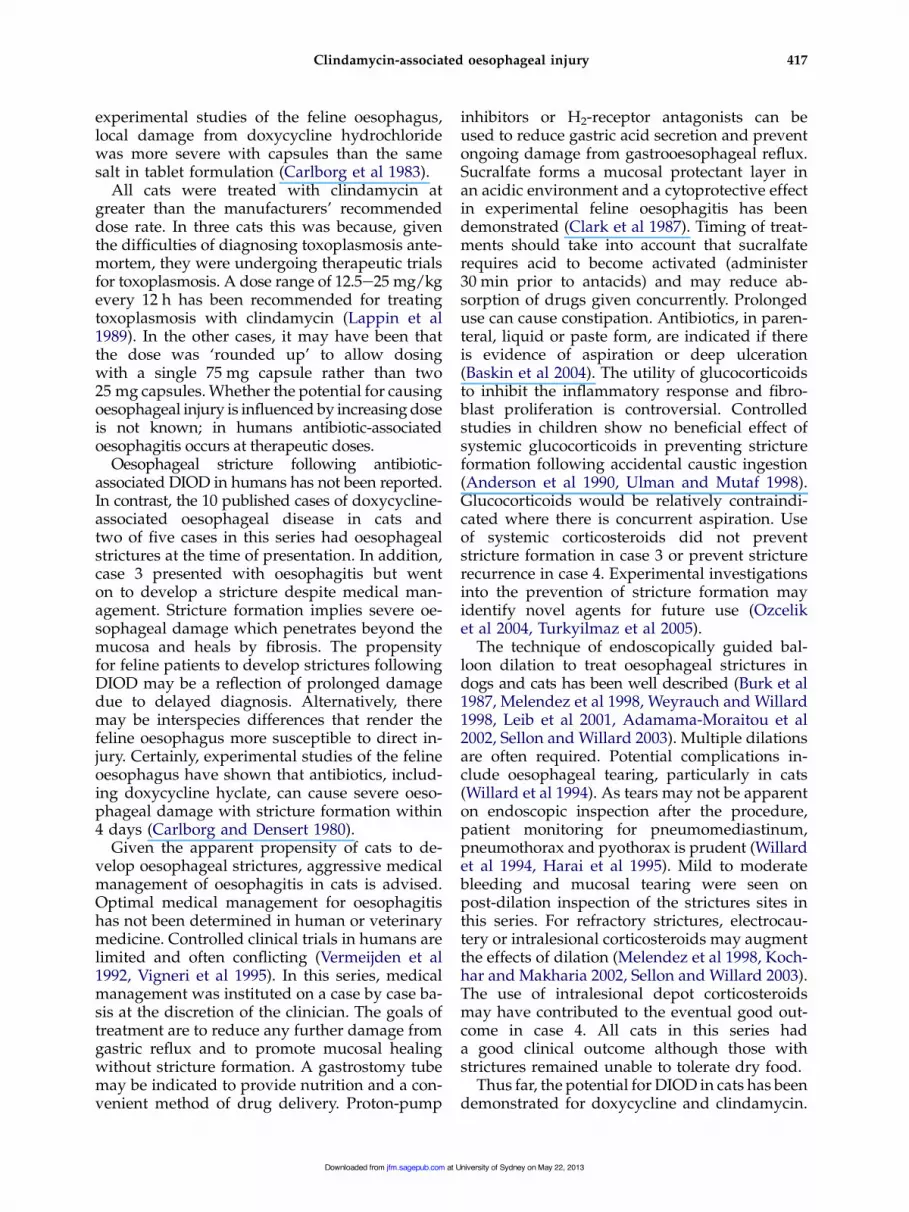
and weight loss. Seventeen days prior topresentation, the cat had been treated for chronic,intermittent bilateral nasal discharge with clinda-mycin hydrochloride capsules (Antirobe; Pfizer)(17 mg/kg per os every 12 h). After 3 days of treat-ment, the cat was noted by the owner, a veterinarystudent, to regurgitate during eating. Treatmentwas stopped but the cat continued to regurgitateand was presented to the Valentine Charlton CatCentre (VCCC). No major abnormalities were de-tected on physical examination, routine haematol-ogy, serum biochemistry or thoracic radiographs.On oesophagoscopy, an area of circumferential,oesophageal ulceration was observed 3e5 cm dis-tal to the proximal oesophageal sphincter (Fig 1).The cat was treated with parenteral prednisolonesodium succinate (Solu Delta Cortef; Pharmacia)(1 mg/kg subcutaneously every 24 h) amoxycillineclavulanate (Clavulox; Pfizer) (14 mg/kg SCevery 12 h), omeprazole (Losec; Astra Zeneca)1 mg/kg intravenously over 1 h every 24 h) for 2days and sucralfate suspension (Carafate; AspenPharmacare) (250 mg PO every 12 h! 7 days).Solids were withheld for 24 h and intravenous*Corresponding author. E-mail: [email protected]
Journal of Feline Medicine and Surgery (2006) 8, 412e419doi:10.1016/j.jfms.2006.04.006
1098-612X/06/060412+08 $32.00/0 ! 2006 ESFM and AAFP. Published by Elsevier Ltd. All rights reserved.
at University of Sydney on May 22, 2013jfm.sagepub.comDownloaded from
fluids were instituted. The next morning the cat re-gurgitated solid food but tolerated liquidisedfood. The cat was discharged on amoxycillineclavulanate oral drops (Clavulox; Pfizer) (12.5 mg/kg every 12 h! 7 days), omeprazole (Losec; AstraZeneca) (1 mg/kg PO every 24 h! 4 days), pred-nisolone (Pred-X5; Apex Labs) (1 mg/kg PO every24 h! 14 days), with instructions to give a 5 mlwater bolus with solid oral medications. Intermit-tent regurgitation was noted during the week fol-lowing discharge. At the time of writing, 5 monthslater, the owner reports that there are no oesopha-geal signs and the cat can tolerate tinned and dryfood.
Case 2
A 1-year-old male neutered Burmese cat pre-sented to the referring veterinarian with a 3-day history of lethargy and anorexia. Pyrexia(40.1(C) was the only abnormality on physicalexamination. Neutropenia (1.8! 109/l; referencerange 3.8e10.1! 109/l) was detected on haema-tology. Serum biochemistry was unremarkable.A Toxoplasma gondii IgG titre was 1280. The catwas hospitalised and supported with intrave-nous fluids. Oral clindamycin (19 mg/kg every12 h! 20 days) was prescribed (day 1). On
days 4 and 5 of hospitalisation, small amountsof undigested food were found in the cat’s cagewithin 15 min of eating. The cat’s appetite anddemeanour gradually improved and it wasdischarged from hospital on day 6 and thenboarded for 2 weeks. The cat was representedto the referring veterinarian 25 days after initialpresentation because it had been unable to toler-ate solid food during boarding. It had lost 12% ofits body weight. The cat was ravenously hungryand was seen to regurgitate solid food immedi-ately after eating. An oesophageal stricture wassuspected. Ranitidine syrup was prescribed(Zantac; GlaxoSmithKline) (2.5 mg PO every12 h) and the cat was referred to the VeterinarySpecialist Centre. On oesophagoscopy, a singlebenign stricture with a lumen of 5 mm wasvisualised 3 cm from the proximal oesophagealsphincter. An 8-mm balloon dilation catheterwas used to dilate the stricture. There was mod-erate post-dilation bleeding and the stricture was1 cm long. Solid food was withheld for 24 h andanalgesia was provided with buprenorphine.Ranitidine syrup was continued and the catwas discharged on amoxycillineclavulanateoral drops (17 mg/kg PO every 12 h! 7 days)and sucralfate suspension (250 mg PO every8 h! 5 days). On oesophagoscopy, 1 week laterthe stricture had partially reformed with a lumenof 7 mm. The dilation procedure was repeatedusing a 12.5-mm balloon. A longitudinal mucosaltear was identified after the dilation. Oesophagi-tis was managed as previously except that dexa-methasone (Dexadreson; Intervet) (0.1 mg/kgSC) was given at the time of dilation and pred-nisolone was give crushed in food (0.8 mg/kgPO every 24 h! 14 days). Two weeks later theowner reported that the cat was able to toleratetinned food but not dry food. Further endoscopywas declined. At 3-month follow-up the cat wasable to tolerate some dry food.
Case 3
A 14-year-old female neutered Burmese cat waspresented to the referring veterinarian withacute, unilateral, peripheral vestibular signs(day 1). Haematology and serum biochemistrywere unremarkable. A T gondii IgG titre was pos-itive (10,240). The cat was treated with clinda-mycin (15 mg/kg PO every 12 h! 10 days).Presenting signs resolved within 12 h. On day4, the owners reported that the cat was bringingup solid food during or immediately after eatingbut was able to tolerate liquids. On day 10, the
Fig 1. Oesophagoscopy (Case 1). Circumferential, oesopha-geal ulceration was observed 3 to 5 cm distal to the upperoesophageal sphincter. Focal areas of deeper ulcerationwere associated with moderate haemorrhage.
413Clindamycin-associated oesophageal injury
at University of Sydney on May 22, 2013jfm.sagepub.comDownloaded from
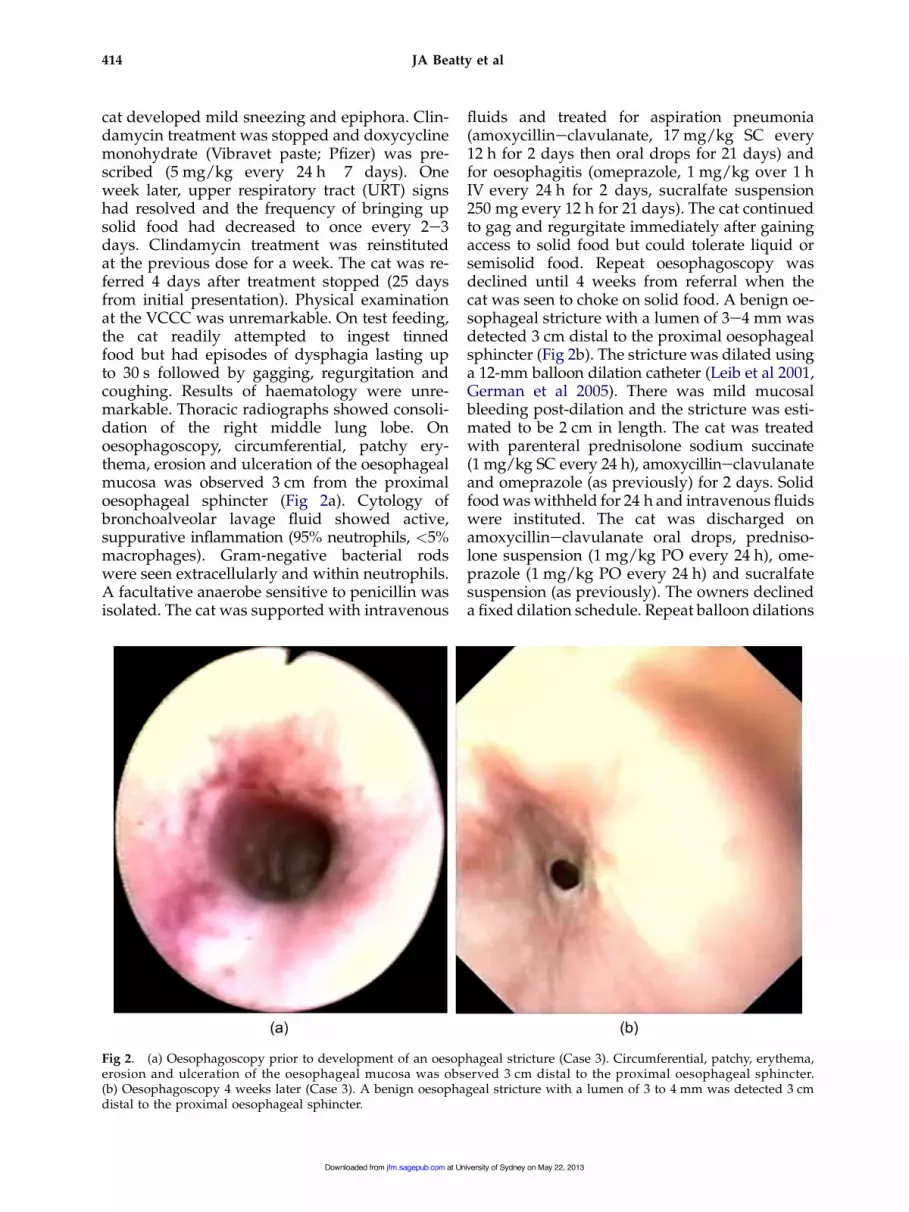
cat developed mild sneezing and epiphora. Clin-damycin treatment was stopped and doxycyclinemonohydrate (Vibravet paste; Pfizer) was pre-scribed (5 mg/kg every 24 h! 7 days). Oneweek later, upper respiratory tract (URT) signshad resolved and the frequency of bringing upsolid food had decreased to once every 2e3days. Clindamycin treatment was reinstitutedat the previous dose for a week. The cat was re-ferred 4 days after treatment stopped (25 daysfrom initial presentation). Physical examinationat the VCCC was unremarkable. On test feeding,the cat readily attempted to ingest tinnedfood but had episodes of dysphagia lasting upto 30 s followed by gagging, regurgitation andcoughing. Results of haematology were unre-markable. Thoracic radiographs showed consoli-dation of the right middle lung lobe. Onoesophagoscopy, circumferential, patchy ery-thema, erosion and ulceration of the oesophagealmucosa was observed 3 cm from the proximaloesophageal sphincter (Fig 2a). Cytology ofbronchoalveolar lavage fluid showed active,suppurative inflammation (95% neutrophils, <5%macrophages). Gram-negative bacterial rodswere seen extracellularly and within neutrophils.A facultative anaerobe sensitive to penicillin wasisolated. The cat was supported with intravenous
fluids and treated for aspiration pneumonia(amoxycillineclavulanate, 17 mg/kg SC every12 h for 2 days then oral drops for 21 days) andfor oesophagitis (omeprazole, 1 mg/kg over 1 hIV every 24 h for 2 days, sucralfate suspension250 mg every 12 h for 21 days). The cat continuedto gag and regurgitate immediately after gainingaccess to solid food but could tolerate liquid orsemisolid food. Repeat oesophagoscopy wasdeclined until 4 weeks from referral when thecat was seen to choke on solid food. A benign oe-sophageal stricture with a lumen of 3e4 mm wasdetected 3 cm distal to the proximal oesophagealsphincter (Fig 2b). The stricture was dilated usinga 12-mm balloon dilation catheter (Leib et al 2001,German et al 2005). There was mild mucosalbleeding post-dilation and the stricture was esti-mated to be 2 cm in length. The cat was treatedwith parenteral prednisolone sodium succinate(1 mg/kg SC every 24 h), amoxycillineclavulanateand omeprazole (as previously) for 2 days. Solidfood was withheld for 24 h and intravenous fluidswere instituted. The cat was discharged onamoxycillineclavulanate oral drops, predniso-lone suspension (1 mg/kg PO every 24 h), ome-prazole (1 mg/kg PO every 24 h) and sucralfatesuspension (as previously). The owners declineda fixed dilation schedule. Repeat balloon dilations
Fig 2. (a) Oesophagoscopy prior to development of an oesophageal stricture (Case 3). Circumferential, patchy, erythema,erosion and ulceration of the oesophageal mucosa was observed 3 cm distal to the proximal oesophageal sphincter.(b) Oesophagoscopy 4 weeks later (Case 3). A benign oesophageal stricture with a lumen of 3 to 4 mm was detected 3 cmdistal to the proximal oesophageal sphincter.
414 JA Beatty et al
at University of Sydney on May 22, 2013jfm.sagepub.comDownloaded from
were performed when the cat was seen to regurgi-tate on days 9, 23, 35, and 70 from the first dilationprocedure. After the fifth dilation, medicationswere stopped apart from prednisolone (1 mg/kgevery 12 h for 14 days, tapered to every 24 h for7 days, then stopped). At the time of writing,7 months later, the cat tolerated tinned but notdry food.
Case 4
A 6-year-old female neutered Burmese cat wastreated for an anal sac abscess with clindamycin(17 mg/kg PO every 12 h for 14 days). Nine daysafter clindamycin treatment began dysphagiawas noted. The cat had a normal appetite buthad difficulty swallowing and brought up undi-gested food during or immediately after eating.Liquidised foods were tolerated. No abnormali-ties were seen on plain thoracic radiographstaken 1 month from the beginning of treatmentwith clindamycin. A barium series showed nor-mal gastric emptying. The cervical oesophaguswas not included in this study. A small amountof barium was aspirated and amoxycillineclavulanate tablets (14 mg/kg PO every 12 h for3 days) were prescribed. The cat was unable tokeep the tablets down so medication waschanged to doxycycline monohydrate paste(5 mg/kg PO every 24 h for 10 days) whichwas tolerated. The cat was referred to the AnimalReferral Hospital, 2 months from the onset ofsigns. On oesophagoscopy, a benign circumfer-ential stricture with a lumen of 3 mm was identi-fied 4 cm distal to the proximal oesophagealsphincter. The stricture was dilated using a 16-mm balloon dilation catheter and a gastrostomytube was placed. Dexamethasone was given(0.1 mg/kg IV). Other medications given paren-terally after the first dilation were cephazolin,ranitidine and metoclopramide. Dilations werecarried out three times weekly initially and thefrequency was gradually reduced. Eleven dila-tions were performed in total over a 14-weekperiod. At the last two dilation procedures,depot methylprednisolone acetate (10 mg)(Depo-Medrol; Pharmacia) was injected radiallyinto the submucosa at the stricture site. Onfinal endoscopy, the oesophageal lumen was8e10 mm at the stricture site. The residual stric-ture was seen as a focal band traversing 180(of the oesophageal lumen. The gastrostomytube was removed. The cat continues to do wellbut is unable to tolerate dry food at 4-monthfollow-up.
Case 5
A 3-year-old female neutered domestic shorthaircat was presented to referring veterinarian witha 10-day history of intermittent lethargy andinappetence. Pyrexia (40.5(C) was detected onphysical examination. No major abnormalitieswere detected on haematology, serum biochem-istry or plain thoracic and abdominal radio-graphs. Serology for feline leukaemia virus,feline immunodeficiency virus and cryptococcalantigen were negative. Supportive treatment withintravenous fluids and amoxycillineclavulanatetablets (14 mg/kg PO every 12 h for 7 days)was initiated. The cat was discharged from thehospital 4 days after admission, on amoxycillineclavulanate and orbifloxacin (2.5 mg/kg POevery 24 h for 5 days). Titres for T gondii IgGand IgM were >2560 and 32, respectively. Threedays later, clindamycin (14 mg/kg PO every 12 h)was prescribed, and amoxycillineclavulanatewas stopped. Seven days after starting clindamy-cin the cat was seen to regurgitate food anda small amount of fresh blood and was referred.On physical examination at the VCCC, mildpyrexia (39.4(C) and generalised joint pain wereidentified. On oesophagoscopy two focal areas ofmucosal erythema and erosion were identified inthe caudal oropharynx adjacent to and involvingthe proximal oesophageal sphincter. Oral medi-cations were withdrawn. The cat was supportedwith intravenous fluids and omeprazole and oralsucralfate suspension. A repeat T gondii IgM titrewas 128. Clindamycin was given intravenously(12.5 mg/kg every 12 h) for suspected toxo-plasmosis. No further oesophageal signs werenoted.
DiscussionDIOD are commonly recognised in humans andare likely to be underreported (Jaspersen 2000,Petersen and Jaspersen 2003, Kadayifci et al2004). More than 70 medications have been impli-cated and over half of all cases involve antibioticadministration (Levine 1999). Doxycycline, clin-damycin and trimethoprimesulphonamide aremost commonly implicated (Sutton and Gosnold1977, Froese 1979, Boyce 1998, Rivera Vaquerizoet al 2004). Antibiotic-associated oesophagitis oc-curs in patients with no pre-existing structural orfunctional oesophageal abnormalities (Bokey andHugh 1975). A history of taking medications withan inadequate volume of liquid immediatelyprior to becoming recumbent is typical. Recum-bency increases oesophageal contact time and
415Clindamycin-associated oesophageal injury
at University of Sydney on May 22, 2013jfm.sagepub.comDownloaded from
increases the chance of gastrooesophageal reflux,while sleep reduces salivation and swallowing(Petersen and Jaspersen 2003). Signs of DIODare typically acute and severe. The most commonsigns are marked odynophagia and retrosternalpain, which occur within hours to days after in-gestion (Boyce 1998). The diagnosis is usuallymade from a consistent history and clinical signsand, in an otherwise healthy patient, endoscopy isgenerally considered unnecessary (Levine 1999,Jaspersen 2000). Oesophagitis is usually mildand self-limiting and resolves on withdrawal ofmedication, although liquid or parenteral analge-sics and medical management may be prescribed(Boyce 1998).
In the veterinary literature, antibiotic-associ-ated oesophageal injury has been documented incats treated with doxycycline hyclate (hydrochlo-ride). All 10 cases had oesophageal strictures at thetime of diagnosis (Melendez et al 2000, Leib et al2001, McGrotty and Knottenbelt 2002, Germanet al 2005). DIOD have not been reported in thedog. In a study of balloon dilation of benign oeso-phageal strictures in dogs and cats, clindamycin isreported as a possible inciting cause but no clinicaldetails are provided (Leib et al 2001). The casespresented here represent the first published clinicalreports of suspected clindamycin-associatedoesophageal injury in cats.
The oesophageal injuries reported in this caseseries most likely result from the administrationof clindamycin capsules by dry swallow. Thetiming of the onset of signs related to treatmentand the absence of evidence of other causes ofoesophageal injury are consistent with this. Inno case was there a history of oesophageal signsprior to the administration of clindamycin. Nounderlying disorder was identified that mightpredispose to increased oesophageal transittime. Furthermore, clindamycin is a knowncause of DIOD in humans (Sutton and Gosnold1977, Froese 1979, Rivera Vaquerizo et al 2004)and the propensity of cats to develop antibiotic-associated oesophageal injury has been docu-mented. The resolution of oesophageal signs intwo of five cases after withdrawal of medicationand medical management for oesophagitis is alsocompelling. In cases 1e4, clindamycin was theonly oral medication given prior to the onset ofsigns. Two cases (cases 3 and 4) received oralmedications in addition to clindamycin. In thesecases, doxycycline and amoxycillineclavulanatewere given after the onset of signs and thus areunlikely to have initiated the lesions but a rolein maintenance or progression of the lesion
cannot be ruled out. However, it should be notedthat the veterinary preparation of doxycyclineavailable in Australia, doxycycline monohydrate(Vibravet; Pfizer) has minimal propensity tocause DIOD compared with the hydrochloride(or hyclate) commonly used in the United King-dom and North America, with one unconfirmedcase on file since 1993 (Trumble 2005). In case 5,oral amoxycillineclavulanate and orbifloxacinhad also been administered in the 2 weeks pre-ceding documentation of mucosal ulceration.An initiating role for these medications cannotbe completely ruled out.
Comparative data on the mechanisms in-volved in the pathogenesis of DIOD in humansare relevant to the cat as the gross anatomy offeline and human oesophagus are similar(Geisinger et al 1990). Furthermore, the use ofthe feline oesophagus as an experimental modelfor human DIOD provides specific informationregarding this species. Prolonged oesophagealcontact in combination with a direct injuriouseffect on the oesophageal mucosa is important;parenteral medications do not cause oesophagealinjury. Some medications are highly irritant. Forexample, potassium chloride can cause oesopha-geal perforation in human patients even in itsliquid form (Pemberton 1970). In contrast, oeso-phageal damage caused by antibiotics in humansis usually restricted to mild erosion and ulcera-tion. Some antibiotics implicated in DIOD havea local irritant effect. Doxycycline hydrochlorideproduces an acidic solution in the normallyneutral pH of oesophagus (Boyce 1998) and itsulcerogenic potential in the feline oesophagushas been demonstrated (Carlborg et al 1983).Clindamycin, however, does not alter oesopha-geal pH (Jaspersen 2000) and clindamycin hydro-chloride solution is minimally irritant in a rabbitcornea model (Pfizer, data on file). Compoundswhich cause minimal local irritation can causeproblems if they are in prolonged mucosal con-tact. The latter may be promoted by dry swallowor capsule formulation. Westfall et al (2001) re-ported that capsules given to cats by dry swal-low were retained in the cervical oesophagus(88%) or oropharynx (8%). In another study,more than 50% of capsules given to normal catsbecame entrapped in the mid-cervical oesopha-gus (Graham et al 2000). This is consistent withour finding that the lesions were located in theproximal oesophagus in the cases presentedhere. Capsules are more likely to be retainedthan tablets and are harder to dislodge onceadhered (Perkins et al 1999, Jaspersen 2000). In
416 JA Beatty et al
at University of Sydney on May 22, 2013jfm.sagepub.comDownloaded from
experimental studies of the feline oesophagus,local damage from doxycycline hydrochloridewas more severe with capsules than the samesalt in tablet formulation (Carlborg et al 1983).
All cats were treated with clindamycin atgreater than the manufacturers’ recommendeddose rate. In three cats this was because, giventhe difficulties of diagnosing toxoplasmosis ante-mortem, they were undergoing therapeutic trialsfor toxoplasmosis. A dose range of 12.5e25 mg/kgevery 12 h has been recommended for treatingtoxoplasmosis with clindamycin (Lappin et al1989). In the other cases, it may have been thatthe dose was ‘rounded up’ to allow dosingwith a single 75 mg capsule rather than two25 mg capsules. Whether the potential for causingoesophageal injury is influenced by increasing doseis not known; in humans antibiotic-associatedoesophagitis occurs at therapeutic doses.
Oesophageal stricture following antibiotic-associated DIOD in humans has not been reported.In contrast, the 10 published cases of doxycycline-associated oesophageal disease in cats andtwo of five cases in this series had oesophagealstrictures at the time of presentation. In addition,case 3 presented with oesophagitis but wenton to develop a stricture despite medical man-agement. Stricture formation implies severe oe-sophageal damage which penetrates beyond themucosa and heals by fibrosis. The propensityfor feline patients to develop strictures followingDIOD may be a reflection of prolonged damagedue to delayed diagnosis. Alternatively, theremay be interspecies differences that render thefeline oesophagus more susceptible to direct in-jury. Certainly, experimental studies of the felineoesophagus have shown that antibiotics, includ-ing doxycycline hyclate, can cause severe oeso-phageal damage with stricture formation within4 days (Carlborg and Densert 1980).
Given the apparent propensity of cats to de-velop oesophageal strictures, aggressive medicalmanagement of oesophagitis in cats is advised.Optimal medical management for oesophagitishas not been determined in human or veterinarymedicine. Controlled clinical trials in humans arelimited and often conflicting (Vermeijden et al1992, Vigneri et al 1995). In this series, medicalmanagement was instituted on a case by case ba-sis at the discretion of the clinician. The goals oftreatment are to reduce any further damage fromgastric reflux and to promote mucosal healingwithout stricture formation. A gastrostomy tubemay be indicated to provide nutrition and a con-venient method of drug delivery. Proton-pump
inhibitors or H2-receptor antagonists can beused to reduce gastric acid secretion and preventongoing damage from gastrooesophageal reflux.Sucralfate forms a mucosal protectant layer inan acidic environment and a cytoprotective effectin experimental feline oesophagitis has beendemonstrated (Clark et al 1987). Timing of treat-ments should take into account that sucralfaterequires acid to become activated (administer30 min prior to antacids) and may reduce ab-sorption of drugs given concurrently. Prolongeduse can cause constipation. Antibiotics, in paren-teral, liquid or paste form, are indicated if thereis evidence of aspiration or deep ulceration(Baskin et al 2004). The utility of glucocorticoidsto inhibit the inflammatory response and fibro-blast proliferation is controversial. Controlledstudies in children show no beneficial effect ofsystemic glucocorticoids in preventing strictureformation following accidental caustic ingestion(Anderson et al 1990, Ulman and Mutaf 1998).Glucocorticoids would be relatively contraindi-cated where there is concurrent aspiration. Useof systemic corticosteroids did not preventstricture formation in case 3 or prevent stricturerecurrence in case 4. Experimental investigationsinto the prevention of stricture formation mayidentify novel agents for future use (Ozceliket al 2004, Turkyilmaz et al 2005).
The technique of endoscopically guided bal-loon dilation to treat oesophageal strictures indogs and cats has been well described (Burk et al1987, Melendez et al 1998, Weyrauch and Willard1998, Leib et al 2001, Adamama-Moraitou et al2002, Sellon and Willard 2003). Multiple dilationsare often required. Potential complications in-clude oesophageal tearing, particularly in cats(Willard et al 1994). As tears may not be apparenton endoscopic inspection after the procedure,patient monitoring for pneumomediastinum,pneumothorax and pyothorax is prudent (Willardet al 1994, Harai et al 1995). Mild to moderatebleeding and mucosal tearing were seen onpost-dilation inspection of the strictures sites inthis series. For refractory strictures, electrocau-tery or intralesional corticosteroids may augmentthe effects of dilation (Melendez et al 1998, Koch-har and Makharia 2002, Sellon and Willard 2003).The use of intralesional depot corticosteroidsmay have contributed to the eventual good out-come in case 4. All cats in this series hada good clinical outcome although those withstrictures remained unable to tolerate dry food.
Thus far, the potential for DIOD in cats has beendemonstrated for doxycycline and clindamycin.
417Clindamycin-associated oesophageal injury
at University of Sydney on May 22, 2013jfm.sagepub.comDownloaded from
These drugs are extremely useful in feline medi-cine and should not be avoided. Prevention ofDIOD in cats can be achieved by a change in dos-ing practices. Careful instructions to give a smallamount of food or a 5e6 ml water bolus with solidoral medications should be given (Graham et al2000, Westfall et al 2001). The contents of clinda-mycin capsules can be combined with a smallamount of food without affecting absorption ofthe drug or the palatability of the food (Pfizer,personal communication, 2005). These instructionsshould be extended to all solid oral medications incats given the wide range of medications that isassociated with DIOD in humans.
AcknowledgementsThe authors are grateful to Drs Stephanie Arm-strong, Antony Kery, Romy Feldman andEmma Holmes-Walker for their role in the clini-cal management of these cases.
AD (2002) Benign esophageal stricture in the dog andcat: a retrospective study of 20 cases. Canadian Journal ofVeterinary Research 66, 55e59.
Anderson KD, Rouse TM, Randolph JG (1990) A controlled trialof corticosteroids in children with corrosive injury of theesophagus. New England Journal of Medicine 323, 637e640.
Baskin D, Urganci N, Abbasoglu L, Alkim C, Yalcin M,Karadag C, Sever N (2004) A standardised protocol forthe acute management of corrosive ingestion in children.Pediatric Surgery International 20, 824e828.
Bokey L, Hugh TB (1975) Oesophageal ulceration associatedwith doxycycline therapy. Medical Journal of Australia 1,236e237.
Burk RL, Zawie DA, Garvey MS (1987) Balloon catheterdilation of intramural esophageal strictures in the dogand cat: a description of the procedure and a report ofsix cases. Seminars in Veterinary Medicine and Surgery (SmallAnimal) 2, 241e247.
Carlborg B, Densert O (1980) Esophageal lesions caused byorally administered drugs. An experimental study in thecat. European Surgical Research 12, 270e282.
Carlborg B, Densert O, Lindqvist C (1983) Tetracyclineinduced esophageal ulcers. A clinical and experimentalstudy. Laryngoscope 93, 184e187.
Clark S, Katz PO, Wu WC, Geisinger KR, Castell DO (1987)Comparison of potential cytoprotective action of sucral-fate and cimetidine. Studies with experimental felineesophagitis. American Journal of Medicine 83, 56e60.
Froese EH (1979) Oesophagitis with clindamycin. SouthAfrican Medical Journal 56, 826.
Geisinger KR, Cassidy KT, Nardi R, Castell DO (1990) Thehistologic development of acid-induced esophagitis inthe cat. Modern Pathology 3, 619e624.
German AJ, Cannon MJ, Dye C, Booth MJ, Pearson GR, ReayCA, Gruffydd-Jones TJ (2005) Oesophageal strictures incats associated with doxycycline therapy. Journal of FelineMedicine and Surgery 7, 33e41.
Graham JP, Lipman AH, Newell SM, Roberts GD (2000)Esophageal transit of capsules in clinically normal cats.American Journal of Veterinary Research 61, 655e657.
Harai BH, Johnson SE, Sherding RG (1995) Endoscopicallyguided balloon dilatation of benign esophageal stricturesin 6 cats and 7 dogs. Journal of Veterinary Internal Medicine9, 332e335.
Jaspersen D (2000) Drug-induced oesophageal disorders:pathogenesis, incidence, prevention and management.Drug safety: An International Journal of Medical Toxicologyand Drug Experience 22, 237e249.
Kadayifci A, Gulsen MT, Koruk M, Savas MC (2004)Doxycycline-induced pill esophagitis. Diseases of theEsophagus 17, 168e171.
Kirkendall JW (1999) Pill esophagitis. Journal of ClinicalGastroenterology 28, 298e305.
Kochhar R, Makharia GK (2002) Usefulness of intralesionaltriamcinolone in treatment of benign esophageal stric-tures. Gastrointestinal Endoscopy 56, 829e834.
Lappin MR, Greene CE, Winston S, Toll SL, Epstein MR(1989) Clinical feline toxoplasmosis. Serologic diagnosisand therapeutic management of 15 cases. Journal of Veteri-nary Internal Medicine 3, 139e143.
Leib MS, Dinnel H, Ward DL, Reimer ME, Towell TL, MonroeWE (2001) Endoscopic balloon dilation of benign esophagealstrictures in dogs and cats. Journal of Veterinary InternalMedicine 15, 547e552.
Levine MS (1999) Drug-induced disorders of the esophagus.Abdominal Imaging 24, 3e8.
McGrotty YL, Knottenbelt CM (2002) Oesophageal stricturein a cat due to oral administration of tetracyclines. Journalof Small Animal Practice 43, 221e223.
Melendez LD, Twedt DC, Weyrauch EA, Millard MD (1998)Conservative therapy using balloon dilation for intramu-ral, inflammatory esophageal strictures in dogs and cast:a retrospective study of 23 cases (1987e1997). EuropeanJournal of Comparative Gastroenterology 3, 31e36.
Melendez L, Twedt D, Wright M (2000) Suspecteddoxycycline-induced esophagitis with esophageal stric-ture formation in three cats. Feline Practice 28, 10e12.
Ozcelik MF, Pekmezci S, Saribeyoglu K, Unal E, GumustasK, Dogusoy G (2004) The effect of halofuginone, a specificinhibitor of collagen type 1 synthesis, in the prevention ofesophageal strictures related to caustic injury. AmericanJournal of Surgery 187, 257e260.
Pemberton J (1970) Oesophageal obstruction and ulcerationcaused by oral potassium therapy. British Heart Journal32, 267e268.
Perkins AC, Wilson CG, Frier M, Vincent RM, Blackshaw PE,Dansereau RJ, Juhlin KD, Bekker PJ, Spiller RC (1999)Esophageal transit of risedronate cellulose-coated tabletand gelatin capsule formulations. International Journal ofPharmaceutics 186, 169e175.
Petersen KU, Jaspersen D (2003) Medication-inducedoesophageal disorders. Expert Opinion on Drug Safety 2,495e507.
Rivera Vaquerizo PA, Santisteban Lopez Y, Blasco Col-menarejo M, Vicente Gutierrez M, Garcia Garcia V,Perez-Flores R (2004) Clindamycin-induced esophagealulcer. Revista Espanola de Enfermedades Digestivas 96,143e145.
418 JA Beatty et al
at University of Sydney on May 22, 2013jfm.sagepub.comDownloaded from
Sellon RK, Willard MD (2003) Esophagitis and esophagealstrictures. Veterinary Clinics of North America, Small AnimalPractice 33, 945e967.
Sutton DR, Gosnold JK (1977) Oesophageal ulceration due toclindamycin. British Medical Journal 1 (6076), 1598.
Trumble C (2005) Oesophageal stricture in cats associatedwith use of the hyclate (hydrochloride) salt of doxycy-cline. Journal of Feline Medicine and Surgery 7, 241e242.
Turkyilmaz Z, Sonmez K, Demirtola A, Karabulut R, PoyrazA, Gulen S, Dincer S, Basaklar AC, Kale N (2005) Mitomy-cin C prevents strictures in caustic esophageal burns inrats. Journal of Surgical Research 123, 182e187.
Ulman I, Mutaf O (1998) A critique of systemic steroids inthe management of caustic esophageal burns in children.European Journal of Pediatric Surgery 8, 71e74.
Vermeijden JR, Tytgat GN, Schotborgh RH, Dekker W, vdBoomgaard DM, van Olffen GH, Schrijver M, VosmaerGD, Dekkers CP (1992) Combination therapy of sucralfate
and ranitidine, compared with sucralfate monotherapy,in patients with peptic reflux esophagitis. ScandinavianJournal of Gastroenterology 27, 81e84.
Vigneri S, Termini R, Leandro G, Badalamenti S, PantalenaM, Savarino V, Di Mario F, Battaglia G, Mela GS, PilottoA, Plebani M, Giovanni D (1995) A comparison of fivemaintenance therapies for reflux esophagitis. New EnglandJournal of Medicine 333, 1106e1110.
Westfall DS, Twedt DC, Steyn PF, Oberhauser EB, VanCleaveJW (2001) Evaluation of esophageal transit of tablets andcapsules in 30 cats. Journal of Veterinary Internal Medicine15, 467e470.
Weyrauch EA, Willard MD (1998) Esophagitis and benignesophageal strictures. Compendium of Continuing Educationfor the Practicing Veterinarian 20, 203e212.
Willard MD, Delles EK, Fossum TW (1994) Iatrogenic tearsassociated with ballooning of esophageal strictures. Jour-nal of the American Animal Hospital Association 30, 431e435.
419Clindamycin-associated oesophageal injury
at University of Sydney on May 22, 2013jfm.sagepub.comDownloaded from