7illet; ~ts, Danny Villalobos, BS Pharm, Edward P. Krenzelok, PharmD, Bruce D. Anderson, PharmD, Susan E. Gorman, PharmD, S. Rutberfoord Rose, PharrnD, June Fenn, BSN, Deborah L. Anderson, ~harmD, Scott J. Muir, BSN, and George C. Rodgers, J~, roD, PhD
Objective: Sixty-eight percent of pediatric sulfonylurea ingestions reported to poison
centers do not result in laboratory or behavioral effects. Consequently, if all exposed
children are admitted overnight or for 24 hours for these exposures, it will result in 600
to 700 hospital admissions per year of children who will remain free of symptoms. We
prospectively studied exposures reported to 10 regional poison centers to determine if
it were possible to differentiate those patients who would have symptoms from those
who would remain symptom flee.
Methods: We analyzed all sulfonylurea exposures in children <12 years old reported
to the participating poison centers. Hypoglycemia was defined as blood glucose (BG)
concentration <60 mg/clL
Results: Hypoglycemia developed in 56 (50%) of 185 exposed patients. Fifty-four of
the 56 (96%) hypoglycemic patients had development of hypoglycemia within 8 hours
of ingestion. Eighty-seven of the patients were initially managed with oral supplemen-
tation only; in 15 cases, treatment advanced to intravenous administration of glucose or
glucagon with the onset of hypoglycemia. There was no statistical difference in medical
outcome between patients monitored during oral supplementation versus during intra-
venous infusion of dextrose. Ingestions analyzed by time of day did not predict risk of
hypoglycemia. Sufficient data were available for 103 (58%) of the 177 patients who in-
gested glyburide or glipizide to calculate a toxic dose/weight ratio. Of these 103 pa-
tients, 31 of 36 patients who ingested -<0.3 mg/kg remained symptom free, whereas 31
Continued on page 142
Accidental pediatric exposure to sulfonyl- ureas is a common experience. For the 5 years of 1990 through 1994, there were 5812 cases of accidental exposure to sul- fonylureas in children <6 years reported to
poison centers. 15 Despite this apparent common clinical experience with pediatric sulfonylurea exposure, there are only limit- ed published data on pediatric overdose to guide practical decisions on treatment. 6"8
From the Kentucky Regional Poison Center, Louisville, Kentucky; Texas Poison Center Network at Galveston, Galveston, Texas; Pittsburgh Poison Center, Pittsburgh, Pennsylvan&' Maryland Poison Center, Baltimore, Maryland; Georgia Poison Center, Atlanta, Georgia; Carolinas Poison Center, Charlotte, North Caroline,. Utah Poison Control Center, Salt Lake Ci~ 3, Utah; Hennepia Regional Poison Center, Mirweapolis, Minaesotc4 and Mugdle Tennessee Poison Center, Nashville, Tennessee.
The effects of sulfonylurea exposure can in- clude profound hypoglycemia and perma- nent neurologic sequelae. 9"13 The sulfonyl- ureas cause hypoglycemia by stimulating release of preformed insulin from the pan- creas. In a manner similar to glucose, sul- fonlyureas reduce conductance of the adenosine triphosphate--sensitive potassium channel on the beta cells, causing membrane depolarization and release of insulin. 14 The clinical effects seen in overdose are the result of the subsequent hyperinsullnemia and by-
poglycemia. The combination of limited data in pediatric exposures and the potential for severe outcome has resulted in the recom- mendation that all pediatrle patients who ac- cidentally ingest sulfonylurea be admitted for 24 hours of direct medical supervision. 6' 15 However, major clinical effects from these exposures are rare. In fact, up to 69% of ac- cidental sulfonylurea exposures in children <6 years reported to poison centers result in no adverse effects. 3 In the single published study of accidental pediatric sulfonylurea exposure, 72% of children remained symp- tom free. 6 Adherence to the recommenda- tion for 2d-hour observation results in annu- M hospital admissions of 600 to 700 children who will not have symptoms and exposes them to hospital-based errors.lS In response to this concern a prospective study was un- dertaken to determine whether certain fac- tors could safely differentiate which patients would experience symptoms and therefore should be admitted from those patients who would remain symptom-free. Specifically,
141
SPILLER ET AL. THE JOURNAL OF PEDIATRICS JULY 1997
of 67 who ingested more than 0.3 mg/kg had BG concentrations <60 mg/dl (p < 0.005,
95% confidence interval 0.05 to 0.58; sensitivity 86%, specificity 46%).
Conclusion: A lack of onset of hypoglycemia (BG >60 mg/dl) in the first 8 hours after
ingestion is predictive of a benign outcome in accidental pediatric stdfonylurea inges-
tion. Clinical observation of children for onset of hypoglycemia during oral feeding
alone appears safe. Some children with symptoms of hypoglycemia need to receive in-
travenous dextrose therapy. Time of day of ingestion is not predictive of risk of hypo-
glycemia. Finally, at this time it appears inappropriate to use a milligram per kilogram
body weight close as a guide for management decisions. ( J Pediatr 1997; 131:141-6)
we attempted to answer five questions: (1) Is time of day of ingestion predictive of out- come? Would children who ingest a sulfo- nylurea in the evening, as the nighttime fast- ing period begins, be at greater risk than children who ingest the drug in the daytime with the potential for oral intake to maintain normoglycemia? (2) Is there a close/weight ratio predictive of risk? A long-term dosing schedule of ehlorpropamide has been used successfully in children as young as S years old (150 to 400 mg/day) in the treatment of central diabetes insipidus. 16' 17 Were there similar dosages with the other sulfonylureas that would be safe for the patients? (J) Do these children require intravenous infusion of glucose during the clinical observation pe- riod, or can normal glycemic status be main- rained with oral food and snacks? It has been suggested that intravenous infusion of glu- cose stimulates further insulin release from an already hypersensifized pancreas, possi- bly worsening the onset of hypoglycemia. 18 (4) Does lack of symptoms in early hours predict a benign outcome? In one study of simulated overdose (1.45 mg/kg glipizide), onset of hypoglycemia occurred within S0 to 165 minutes. 18 (5) Do all children who in- gest sulfonylureas need 24 hours of hospital observation as previously recommended?
METHODS
This was a 1-year observational pro- spective case series of accidental sulfo- nylurea exposure in children _<12 years whose cases were reported to 10 regional poison centers serving a population of ap- proximately 37 million. Data were collect- ed from September 1994 to August 1995.
The data collected included age, gender, drug and dose ingested, time of ingestion, clinical effects including frequent blood glucose monitoring, type of glucose moni- toring (i.e., venipuncture vs finger stick), onset and duration of any clinical effects, any therapies instituted, effect of thera- pies, duration of hospital stay, and medical outcome. Treatment and disposition rec- ommendations that were offered by the in- dividual participating poison centers were not altered by entrance into the study. For the purposes of this study hypoglycemia was defined as a BG concentration of <60 mg/dl (3.3 mmol/L). Blood samples for glucose measurements were obtained by either venipuncture or finger stick method, at the discretion of the treating fa- cility. Statistical analysis of dose/weight ratio was by chi square. Analysis of vari- ance was used to analyze the relation of time of ingestion to incidence of hypo- glycemia. Medical outcome was defined according to the following: (1) no effect~ BG concentration remained ->60 mg/dl and the patient had no symptoms; (2) minor effect--at least one BG measure- ment was below 60 mg/dl, but the patient experienced no apparent clinical effects; (3) moderate effect--at least one BG mea- surement was below 60 mg/cll, and the pa- tient experienced associated systemic clin- ical effects such as diaphoresis, agitation, or lethargy" but symptoms did not require specific intervention beyond administra- tion of glucose; (4) major e f fec t -a t least one BG measurement was below 60 mg/dl, and the patient experienced associ- ated, more serious systemic effects such as a seizure or coma that required specific medical intervention. Approval of this
study was granted by the University of Louisville, School of Medicine, University Human Studies Committee.
RESULTS
One hundred and eighty-five cases of accidental sulfonylurea ingestion were documented. Age of patients rafiged from 10 months to 11 years, with a mean of 2.4 years (SD ± 1.7 years). The cases were evenly distributed between the sexes with 97 male subjects (52%). A total of 180 pa- tients received direct medical evaluation and 161 (870/0) were admitted for obser- vation. Mean hospital stay was 23.6 hours (SD ± 1.05 hours). Mean hospital stays for those with and without hypoglycemia were 28.2 (SD ± 2.3) and 21.6 hours (SD ± 1.1), respectively. In five cases, patients were followed at home with finger stick checks made by the parent. All five re- mained symptom-free and none had a BG concentration <60 mg/dl. All cases were followed up for at least 24 hours. No pa- tients had seizures or coma in this study.
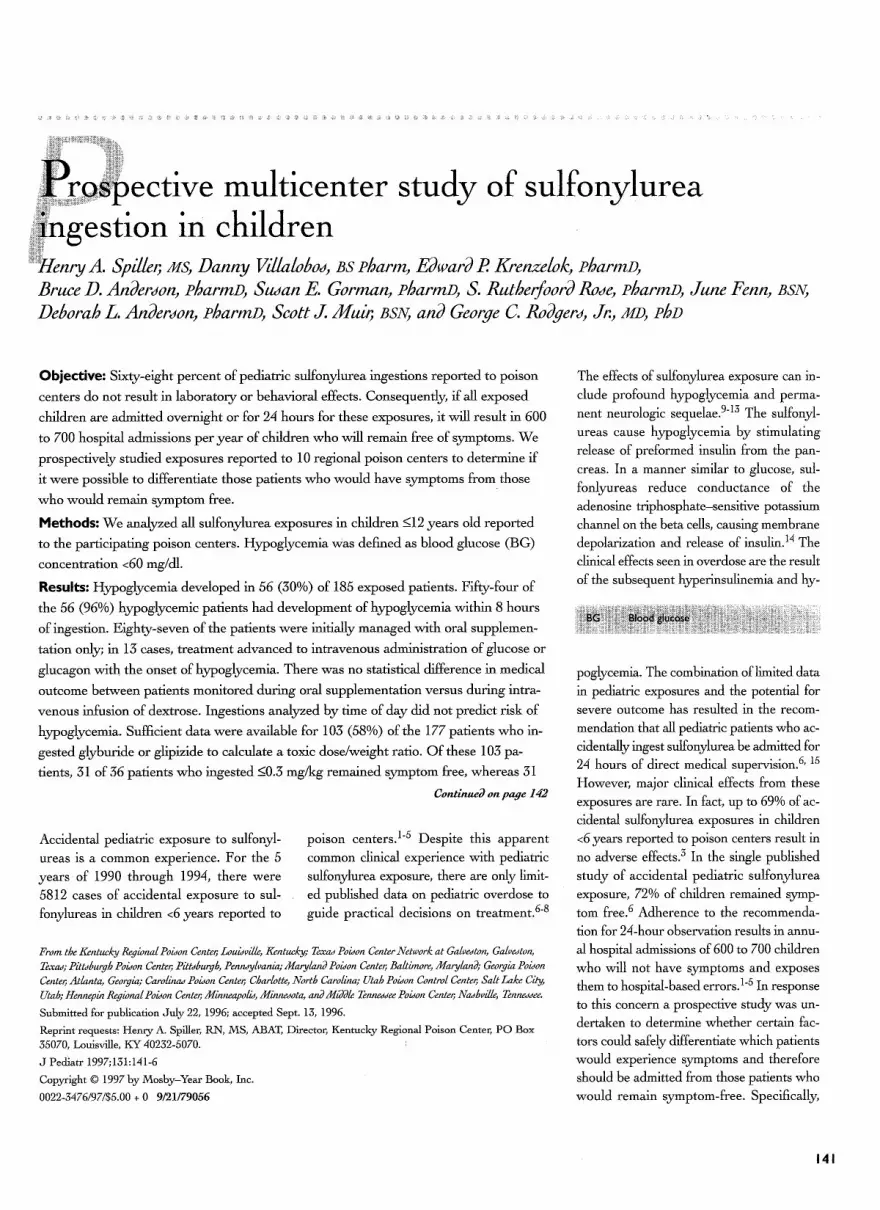
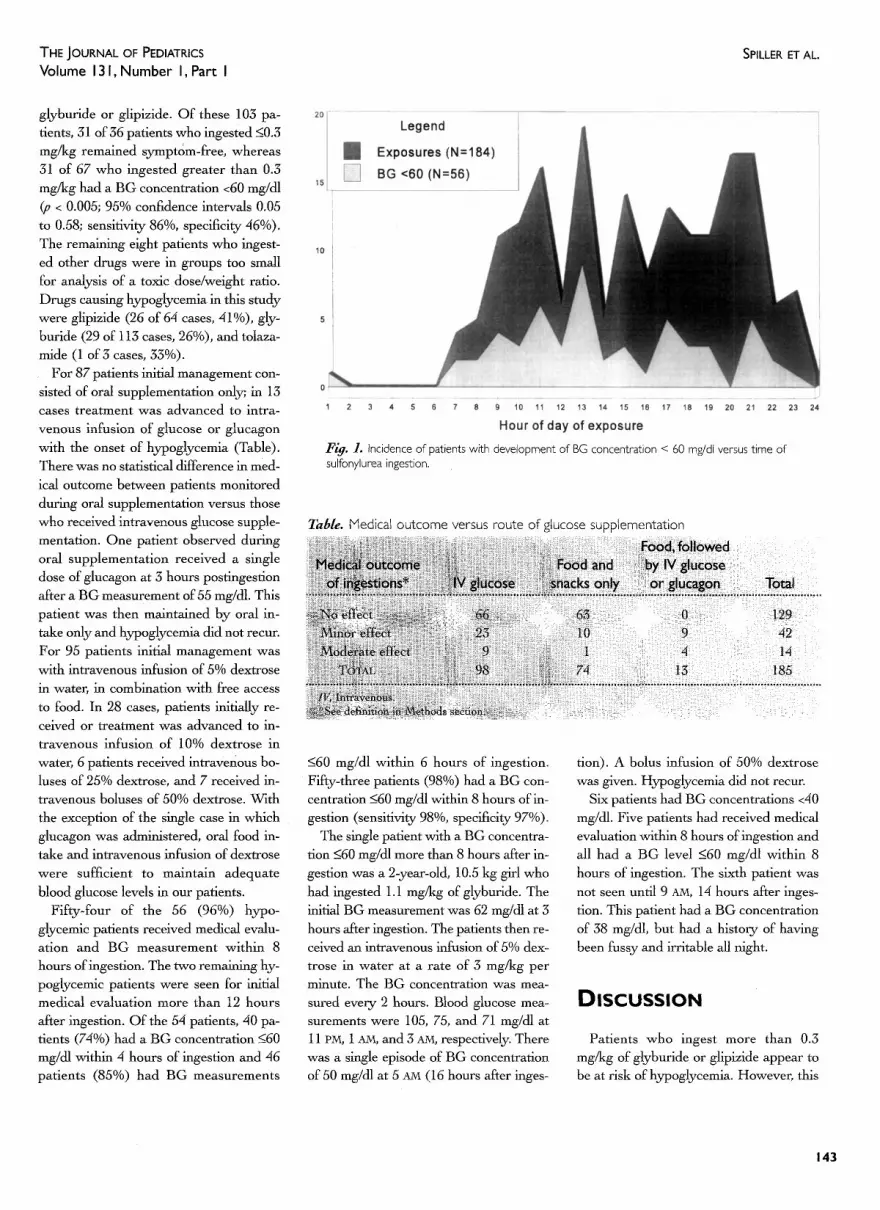
Fifty-six patients (30%) had BG con- centrations <60 mg/dl, and 6 cases (3%) had BG measurements <40 mg/dl. The minimum recorded glucose concentration was 33 mg/dl. The mean minimum BG for those patients with and without hypo- glycemia was 49.5 (SD ± 6.4) and 78.8 (SD ± 12.9), respectively. The mean time after ingestion to the minimum BG level in those patients with hypoglycemia was 5.3 hours (SD ± 4.8) with a range of 1 to 21 hours. The median and mode hours to minimum glucose were 3.2 and 2 hours, respectively. Time of day of ingestion was known for 184 patients. No correlation was found between time of day of inges- tion and incidence of hypoglycemia (Fig. 1). Hour of day nadir of hypoglycemia in those patients with BG measurements <60 mg/dl is presented in Fig. 2.
Drugs ingested included glyburide (n = 113), glipizide (n = 64), chlorpropamide (n = 4), tolazamide (n = 3), and gliclazide (n = 1). Sufficient data were available to calculate a dose/weight ratio for 103 (58%) of the 177 patients who ingested
142
THE JOURNAL OF PEDIATRICS Volume 13 I, N u m b e r I, Part I
SPILLER ET AL.
glyburide or glipizide. Of these 103 pa- rents, 31 of 36 patients who ingested <_0.3 mg/kg remained symptom-free, whereas 31 of 67 who ingested greater than 0.3 mg/kg had a BG concentration <60 mg/cll (p < 0.005; 95% confidence intervals 0.05 to 0.58; sensitivity 86%, specificity 46%). The remaining eight patients who ingest- ed other drugs were in groups too small for analysis of a toxic dose/weight ratio. Drugs causing hypoglycemia in this study were glipizide (26 of 64 cases, 41%), gly- buride (29 of 113 cases, 26%), and tolaza- mide (1 of 3 cases, 33%).
For 87 patients initial management con- sisted of oral supplementation only; in 13 cases treatment was advanced to intra- venous infusion of glucose or glucagon with the onset of hypoglycemia (Table). There was no statistical difference in med- ical outcome between patients monitored during oral supplementation versus those who received intravenous glucose supple- mentation. One patient observed during oral supplementation received a single dose of glucagon at 3 hours postingestion after a BG measurement of 55 mg/dl. This patient was then maintained by oral in- take only and hypoglycemia did not recur. For 95 patients initial management was with intravenous infusion of 5% dextrose in water, in combination with free access to food. In 28 cases, patients initially re- ceived or treatment was advanced to in- travenous infusion of 10% dextrose in water, 6 patients received intravenous bo- luses of 25% dextrose, and 7 received in- travenous boluses of 50% dextrose. With the exception of the single case in which glucagon was administered, oral food in- take and intravenous infusion of dextrose were sufficient to maintain adequate blood glucose levels in our patients.
Fifty-four of the 56 (96%) hypo- glycemic patients received medical evalu- ation and BG measurement within 8 hours of ingestion. The two remaining hy- poglycemic patients were seen for initial medical evaluation more than 12 hours after ingestion. Of the 54 patients, 40 pa- tients (74%) had a BG concentration _<60 mg/dl within 4 hours of ingestion and 46 patients (85%) had BG measurements
F/#. L Incidence of patients with development of BG concentration < 60 mg/dl versus time of sulfonylurea ingestion.
Table. Medical outcome versus route of glucose supplementation
<60 mg/dl within 6 hours of ingestion. Fifty-three patients (98%) had a BG con- centration -<60 mg/dl within 8 hours of in- gestion (sensitivity 98%, specificity 97%).
The single patient with a BG concentra- tion <60 mg/dl more than 8 hours after in- gestion was a 2-year-old, 10.5 kg glrl who had ingested 1.1 mg/kg of glyburide. The initial BG measurement was 62 mg/dl at 3 hours after ingestion. The patients then re- ceived an intravenous infusion of 5% dex- trose in water at a rate of 3 mg/kg per minute. The BG concentration was mea- sured every 2 hours. Blood glucose mea- surements were 105, 75, and 71 mg/dl at 11 p/vi, 1 ~'~, and 3 AM, respectively. There was a si@e episode of BG concentration of 50 mg/dl at 5 AM (16 hours after inges-
tion). A bolus infusion of 50% dextrose was given. Hypoglycemia did not recur.
Six patients had BG concentrations <40 mg/cll. Five patients had received medical evaluation within 8 hours of ingestion and all had a BG level <60 mg/dl within 8 hours of ingestion. The sixth patient was not seen until 9 AM, 14 hours after inges- tion. This patient had a BG concentration of 38 mg/dl, but had a history of having been fussy and irritable all night.
D I S C U S S I O N
Patients who ingest more than 0.3 mg/kg of glyburide or glipizide appear to be at risk of hypoglycemia. However, this
143
SPILLER ET AL. THE JOURNAL OF PEDIATRICS JULY 1997
7
6
5
4
3
2
1
0
3 5 7 9 11 13 15 17 19 21
Patients with hypoglycemia (N=56)
F/g. 2. Hour of day of nadir of hypoglycemia after sulfonylurea ingestion.
23
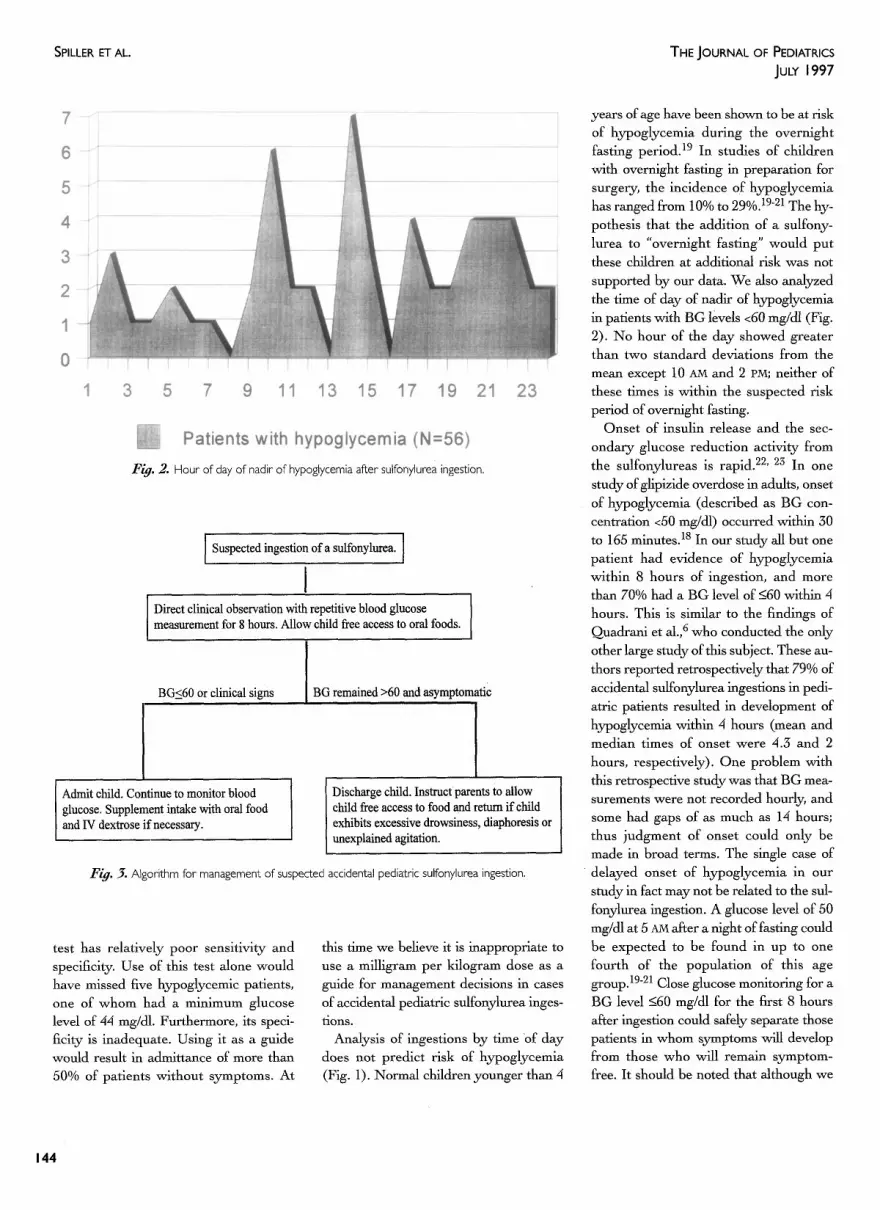
I Suspected ingestion of a sulfonylurea. ]
Direct clinical observation with repetitive blood glucose measurement for 8 hours. Allow child free access to oral foods.
BG<60 or clinical signs BG remained >60 and asymptomafic
I Admit child. Continue to monitor blood glucose. Supplement intake with oral food and IV dextrose if necessary.
Discharge child. Instruct parents to allow child free access to food and return if child exhibits excessive drowsiness, diaphoresis or unexplained agitation.
F/g. 3. Algorithm for management of suspected accidental pediatric sulfonylurea ingestion.
test has relatively poor sensitivity and specificity. Use of this test alone would have missed five hypoglycemlc patients, one of whom had a minimum glucose level of 44 mg/dl. Furthermore, its speci- ficity is inadequate. Using it as a guide would result in admittance of more than 50% of patients without symptoms. At
this time we believe it is inappropriate to use a milligram per kilogram dose as a guide for management decisions in cases of accidental pediatric sulfonylurea inges- tions. Analysis of ingestions by time "of day
does n o t predict risk of hypoglycemia (Fig. 1). Normal children younger than 4
years of age have been shown to be at risk of hypoglycemia during the overnight fasting period. 19 In studies of children with overnight fasting in preparation for surgery, the incidence of hypoglycemia has ranged from 10% to 29%. 1921 The hy- pothesls that the addition of a sulfony- lurea to "overnight fasting" would put these children at additional risk was not supported by our data. We also analyzed the time of day of nadir of hypoglycemia in patients with BG levels <60 mg/dl (Fig. 2). No hour of the day showed greater than two standard deviations from the mean except 10 AM and 2 PM; neither of these times is within the suspected risk period of overnight fasting.
Onset of insulin release and the sec- ondary glucose reduction activity from the sulfonylureas is rapid. 22' 23 In one study of glipizide overdose in adults, onset of hypoglycemia (described as BG con- centration <50 mg/dl) occurred within 30 to 165 minutes. 18 In our study all but one patient had evidence of hypoglycemia within 8 hours of ingestion, and more than 70% had a BG level of -<60 within 4 hours. This is similar to the findings of Ouadrani et al.,6 who conducted the only other large study of this subject. These au- thors reported retrospectively that 79% of accidental sulfonylurea ingestions in pedi- atric patients resulted in development of hypoglycemia within 4 hours (mean and median times of onset were 4.3 and 2 hours, respectively). One problem with this retrospective study was that BG mea- surements were not recorded hourly, and some had gaps of as much as 14 hours; thus judgment of onset could only be made in broad terms. The single case of
d e l a y e d onset of hypoglycemia in our study in fact may not be related to the sul- fonylurea ingestion. A glucose level of 50 mg/cll at 5 AM after a night of fasting could be expected to be found in up to one fourth of the population of this age group. 19-21 Close glucose monitoring for a BG level -<60 mg/cU for the first 8 hours after ingestion could safely separate those patients in whom symptoms ~ l l develop from those who will remain symptom- free. It should be noted that although we
144
THE JOURNAL OF PEDIATRICS Volume 13 I, N u m b e r I, Part I
SPILLER ET AL.
are discussing early onset of action, we would stress that the duration of action of these drugs can be very longfi' 8, 1~, 24 In
our study, one patient in whom hypo- glycemia developed had a nadir of hypo- glycemia at 21 hours after ingestion. We believe patients in whom hypoglycemia develops should continue to be monitored under direct medical supervision foi ~ up to 24 hours.
Finally, it appears that patients may be safely monitored while receiving oral sup- plementation alone during the initial 8- hour observation period. We found no change in outcome when we compared those patients initially managed with oral intake versus those who received intra- venous dextrose therapy. Those patients in whom hypoglycemia develops may then receive more advanced treatment with intravenously administered dextrose, if necessary, and be admitted for observa- tion and treatment.
A limitation of this study is the lack of laboratory confirmation of sulfonylurea ingestion. In a number of cases the inges- tion was an unconfirmed ingestion, with a history of infmate access to the pills dur- ing an unsupervised period. This is a com- mon experience in pediatric poisoning and will likely continue to occur in many such cases in the future. Because the risk of hypoglycemia is severe and may occur with ingestion of a single tablet, in such eases admission for prolonged observa- tion is routinely recommended. 6' 25 In the
absence of confirmatory serum sulfony- lurea levels, the BG concentration, histo- ry, and clinical symptoms are the only fac- tors that remain to help in the management decision. Testing for serum sulfonylurea levels is not widely available, is expensive, and there are no studies to make interpretation of these levels clini- cally useful. Conversely, blood glucose sampling is inexpensive, widely available, and easily interpreted. For this reason we focused on blood glucose measurements in our study.
The analysis of our clara is based heavi- ly on blood glucose measurements versus clinical symptoms of hypoglycemia. Forty-two of our patients had BG mea-
surements < 60 mg/di without evidence of clinical symptoms (Table). However, 32 of these 42 patients were subsequently
treated with intravenous dextrose infu- sions that may have forestalled the onset of clinical symptoms of hypoglycemia, which can include seizures and coma. Of the 14 patients with BG levels <60 mg/di who had hypoglycemia-associated symp- toms, 12 were described as drowsy or lethargic and two were described as fussy or agitated. These symptoms, although re- lated, were considered too nonspecific to use as a basis on which to make patient disposition decisions.
A lack of hypoglycemia (BG concentra- tion -<60 mg/dl) in the first 8 hours after ingestion is predictive of a benign out- come in accidental pediatric sulfonylurea ingestion. Direct clinical observation with repetitive BG testing during the first 8- hour postingestion period is recommend- ed. Observing children for onset of hypo- glycemia while they are receiving only oral foods appears safe. Some children will require more advanced treatment with intravenous dextrose infusions. Time of day of ingestion is not predictive of risk of hypoglycemia. Finally, at this time it appears inappropriate to use a milligram per kilogram dose as a guide for manage- ment decisions.
We thank Maureen Frenia, PharmD, for sup- plying data from cases reported to the Florida Poison Information Center, Jacksonville, Florida.
REFERENCES 1. Litovitz TL, Bailey KM, Schmitz BE Holm
KC, Klein-Swartz W. 1990 annual report of the American Association of Poison Control Centers National Data Collection System. Am J Emerg Med 1991;5:461-509.
2. Litovitz TL, Holm KC, Bailey KM, Schmitz BF. 1991 annual report of the American Association of Poison Control Centers National Data Collection System. Am J Emerg Med 1992;5;452-505.
3. Litovitz TL, Holm KC, Clancy C, Schmitz BE Clark LR and Oderda GM. 1992 annu- M report of American Association of Poison Control Centers Toxic Exposure Surveil- lance System. Am J Emerg Med 1993;11: 494-555.
4. Litovitz TL, Clark LR, Soloway RA. 1993
annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 1994;12:546-84.
5. Litovitz TL, Felberg L, Soloway RA, Ford M, Geller R. 1994 annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 1995;5:551-97.
6. Quadrani DA, Spiller HA, Widder R Five year retrospective evaluation of sulfony- lurea ingestion in children. J Toxicol Clin Toxicol 1996;34:267-70.
7. Erickson T, Arora A, Lebby TI, Lipseomb JW, Leiken JB. Acute oral hypoglycemie ingestions. Vet Hum Toxicol 1991;33:256-8.
8. Palatnick W, Metherall RC, Tenebein M. Clinical spectrum of sulfonylurea overdose and experience with diazoxide therapy. Arch Intern Med 1991;151:1859-62.
13. Pavone L, Molllca F, Musumeci S, Marino S, Pampiglione G. Accidental gliben- clamide ingestion in an infant: clinical and electorencephalographic aspects. Dev Med Child Neurol 1980;22:566-70.
14. Kahn RC, Schecter Y. Insulin, oral hypo- glycemic agents and the pharmacology of the pancreas. In: Gilman AG, Rail TW, Nies AS, Taylor P, editors. Goodman and Oillman's pharmacologic basis of therapeu- tics. 8th ed. New York: Pergamon Press, New York; 1990.
16. Ehrlich RM, Kooh SW. The use of chlor- propamide in diabetes insipidus in children. Pediatrics 1970;45:236-45.
17. Vallet HL, Prasad M, Goldbloom RB. Chlorpropamide treatment of diabetes in- sipidus in children. Pediatrics 1970;45:246- 53.
18. Boyle PJ, Justice K, Krentz A J, NaKg R J, Schade DS. Octrotide reverses hyperinsu- linemia and prevents hypoglycemia induced by sulfonylurea overdose. J Clin Endo- crinol Metab 1993;76:752-6.
19. Thomas DKM. Hypoglycemia in children before operation: its incidence and preven- tion. Br J Anaesth 1974;46:66-8.
20. Watson BG. Blood glucose levels in chil-
145
SPILLER ET AL.
dren during surgery. Br J Anaesth 1972;44:712-5.
21. Bevan JC, Burn MC. Acid base changes and anesthesia: the influence of pre-oper- ative starvation and feeding in pediatric surgical patients. Anesthesia 1975;28:415- 22.
22. Sartor G, Melander A, Schersten B,
23.
Wahlin-Boll E. Comparative single dose ki- netics and effects of four sulfonylureas in healthy volunteers. Acta Med Scand 1980;208:301-7. Brogden RN, Heel RC, Pakes GE, Speight TM, Avery GS. Glipizide: a review of its pharmacological properties and therapeutic use. Drugs 1979;18:529-55.
THE JOURNAL OF PEDIATRICS JULY 1997
24. Jacohs RF, Nix RA, Paulus TE, Keil EA, Fiser RH. Intravenous infusion of diazox- ide in the treatment of chlorpropamide-ln- dueed hypoglycemia. J Pediatr 1978;93: 801-5.
Fellowships available in pediatric subspecialties and those for general academic pediatric training are listed once a year, in January , in The Journal of Pediatrics. Each June, forms for listing fellowships available for the academic year beginning 18 months after publication are sent to the Chairman of the Department of Pediatrics at major hospitals in the United States and Canada. In addition, a copy of the applicat ion form appears in the July, August, and September issues of The Journal (please use the current form). Should you desire to list fel- lowships, a separate application must be made eachyear for each position. All applications must be returned to Mosby-Year Book, Inc., by October 15 preceding the listing year to ensure publication. Addit ional forms will be supplied on request from the Journa l Editing Department, Mosby-Year Book, Inc., 11830 Westline Industrial Drive, St. Louis, M O 63146- 3318 (phone: 800-325-4177, ext. 2838, or 314-579-2838).