1997;128;1253-1261J Am Dent Assoc Bird, S Lowe and JL GerberdingF Ramos-Gomez, J Ellison, D Greenspan, Wclinics: a prospective studyamong health care workers in dental teaching Accidental exposures to blood and body fluids
jada.ada.org ( this information is current as of July 15, 2011):The following resources related to this article are available online at
http://jada.ada.org/content/128/9/1253found in the online version of this article at:
including high-resolution figures, can beUpdated information and services
http://jada.ada.org/cgi/collection/infection_controlInfection Control : subject collectionsThis article appears in the following
http://www.ada.org/990.aspxreproduce this article in whole or in part can be found at:
of this article or about permission toreprintsInformation about obtaining
ACCIDENTALEXPOSURESTO BLOODAND BODYFLUIDSAMONG HEALTH
CAREWIORKERS IN DENTAL TEACHING CLINICS: A PROSPECTIVE STUDYFRANCISCO RAMOS-GOMEZ, D.D.S., M.S., M.P.H.; JAMES ELLISON, D.D.S., M.P.H.; DEBORAHGREENSPAN, B.D.S., D.SC.; WILLIAM BIRD, D.D.S., D.P.H.; SAM LOWE, M.A., R.N.; JULIE LOUISEGERBERDING, M.D., M.P.H.
Wxposure to bloodbornepathogens, including HIV; hep-atitis B virus, or HBV; and hep-atitis C virus, or HCV, is a sig-nificant occupational hazardamong health care workers, andpercutaneous injuries pose thegreatest risk of infection.13 Ithas been difficult to assess therisk of occupationally acquiredinfection for dental workers andother health care providers, be-cause of the complexity, expenseand time involved in collectingthe prospective data. Therefore,most of the available data wereacquired retrospectively.
Estimates based on data fromthe Centers for Disease Controland Prevention, or CDC, andother studies suggest that ahealth care provider's risk of ac-quiring HIV infection as a re-sult of percutaneous exposure toan HIV-contaminated device is0.3 percent.36 The reported riskassociated with HCV exposuresranges from 2.7 percent to 10.0percent, and the risk from HBVexposures ranges from 5.0 per-cent to 45.0 percent.3
Relatively few dental healthcare workers have been includ-ed in the reported studies of oc-cupational risk from exposuresto blood, and the types of in-juries sustained in proceduresperformed in dental practicesdiffer from those sustained inother branches of health care.
The authors evaluated acciden-
tal exposures to blood and body
fluids reported to a hotline or to
health officials at four dental
teaching clinics. The authors
used a standard questionnaire to
solicit and record data regarding
each exposure. During a 63-
month period, 428 parenteral ex-
posures to blood or body fluids
were documented. Dental stu-
dents and dental assistants had
the highest rates of exposure.
Syringe needle injuries were the
most common type of exposure,
while giving injections, cleaning
instruments after procedures
and drilling were the activities
most frequently associated with
exposures.
For example, the position in theoperatory of the dental cart thathas handpieces on the side andthe dental tray containing den-tal burs and sharp instrumentson top can contribute to in-juries. Another factor is the er-gonomics related to the pa-tient/dentist position, whichmight contribute to more in-
juries than those that occur inother health specialties.
The first attempt to assessthe occupational risk of HIV in-fection among dental workerswas reported by Klein and col-leagues, who conducted a sur-vey of 1,309 dental professionalsin New York state.7 The subjectsestimated the number of acci-dental parenteral inoculationsthey had received during thepreceding 5 years. Then serumsamples were taken from eachsubject and tested for antibodiesto HIV. Despite variable adher-ence to infection-control prac-tices among the subjects, occu-pational infection was rare: onlyone of the 1,309 subjects, noneofwhom had behavioral riskfactors for AIDS, had antibodiesto HIV. The risk among subjectspracticing in regions with ahigh incidence ofAIDS caseswas 1 in 673. The limitations ofthis study included the relianceon the subjects' ability to recallexposures and the lack of infor-mation on the types of exposure.
In 1992, Capilouto and col-leagues8 showed that the annualcumulative risk of infection fordentists from routine treatmentof patients whose seropositivityis undisclosed is 57 timesgreater for HBV than that forHIV, and that the risk of dyingas a result of occupational expo-sure to HBV is 1.7 times greater
than that because of occupa-tional exposure to HIV.
Three 1995 studies have pro-vided more specific informationon a small sample of percuta-neous injuries experienced bydental health care workers.Gooch and colleagues9 describedthe circumstances of percuta-neous exposure to HIV-infectedblood among 19 dental workersenrolled in the CDC's Needle-stick Study. The subjects in-curred injuries with scalers,burs, small-gauge hollow-boreneedles and explorers, duringeither use, cleanup, disassem-bly or recapping. The exposuresinvolved relatively smallamounts of blood and did not re-sult in infection.
In an observational study ofdental residents, Cleveland andcolleagues10 reported 14 percu-taneous injuries (1.2 per 1,000patient visits, 0.33 per dentist-month of 136 hours). Eighty-sixpercent of the percutaneous in-juries occurred extraorally, and36 percent occurred while adental resident was using autility knife to trim denture im-pressions.
In a study of 2,304 practicingdentists who recorded injuriesin a daily log for 1 month, Siewand colleagues"l found a meanpercutaneous injury rate of 0.28per dentist-month. Most of thesubjects incurred extraoral in-juries with burs, sharp instru-ments and syringe needles. Allthree above-mentioned studiesconcluded that further informa-tion about the rates and circum-stances of accidental exposuresamong dental health care work-ers was essential.9-11
Our study was designed toevaluate the epidemiology of ex-posures to blood and body fluidsin dental teaching clinics. Since1989, data on exposures to
blood or body fluids at four den-tal teaching clinics in SanFrancisco have been collectedprospectively, using a standardquestionnaire to elicit detailedinformation about each expo-sure. We reviewed the data col-lected between October 1, 1989,and December 31, 1994, to as-sess the frequency of accidentaloccupational exposures to bloodor body fluids among dentalhealth care workers, to charac-terize the circumstances of theexposures and to identify specif-ic ergonomic interventions andother actions that could helpprevent exposures in this typeof setting.
SUBJECTS ANDMETHODS
The subjects in this study wereall dental health care providers,including faculty members, resi-dents, dental students, hygien-ists, dental assistants and staffmembers at four dental teachingclinics in San Francisco. Threeof these clinics were affiliatedwith the dental school at theUniversity of California, SanFrancisco, or UCSF, and oneclinic was affiliated with thedental school at the Universityof the Pacific, or UOP. We in-cluded the following exposuresinvolving blood or body fluids inthe study: percutaneous in-juries, splashes to mucosa (ornonintact skin) and bites.Data reporting and collec-
tion procedures. At the UCSFclinics, dental health care work-ers are required to report all ex-posures to blood or body fluidsto a 24-hour exposure hotline.Instructions for reporting expo-sures are posted in each dentalwork space. During their initialorientation to the clinical areas,dental students and residentsreceive oral instructions on how
to use the hotline. Faculty andstaff receive written explana-tions of the reporting procedure.In addition, all personnel aregiven wallet-sized cards de-scribing the procedure.
Trained clinicians answercalls to the hotline, provide theinitial exposure assessment andarrange for follow-up care. Thetrained clinicians use a standardquestionnaire we developed tosolicit and record basic informa-tion about the incident. This in-formation includes the worker'sname, work area, job classifica-tion, type of exposure (percuta-neous injury, mucous membranecontamination, bite, nonintactskin contamination), exposurecircumstances and source pa-tient information (bloodbornepathogen infections, risk factorsfor infectious diseases).
At the UOP clinic, dental stu-dents are required to reporttheir exposures in person to stu-dent health officials. Facultyand staff are required to reportexposures to employee healthofficials. All clinical personnelare encouraged, through verbalinstructions and written re-minders, to report every expo-sure. A nurse or nurse practi-tioner obtains and documentsthe information from each re-ported exposure using the samequestionnaire that is used atthe UCSF sites.We originally designed this
questionnaire to facilitate expo-sure surveillance and manage-ment among all health care per-sonnel, including dental pro-viders, at San Francisco GeneralHospital. In April 1992, we ex-panded the questionnaire to ob-tain more detailed informationabout exposure mechanisms indental settings than that ob-tained from the original ques-tionnaire.
Follow-up protocol afterexposure. After the question-naire has been completed, thedental health care provider isencouraged by the OccupationalEmployee Health Office to un-dergo a baseline test of HIV,HCV and HBV status. If the ex-posure involved blood from apatient infected with HCV orHIV, the dental health careprovider is encouraged to un-dergo follow-up testing at 6weeks, 12 weeks, 6 months and12 months after the exposure todetect seroconversion. Counsel-ing is offered before and aftertesting. Postexposure treatmentwith antiretroviral therapy isalso available and recommend-ed.12 Whenever possible, thesource patient's blood is evalu-ated for bloodborne pathogenswithin 24 hours after the expo-sure. The source patient isasked to consent to HIV anti-body testing when risk factorsfor HIV are evident; the sourcepatient also receives counselingbefore and after HIV testing,and the results are kept confi-dential. Serologic tests for HBV,and more recently HCV, arealso performed.Data analysis. We deleted
personal identifiers from thequestionnaires and compiled andanalyzed the data using Epi-Info,Version 5.01b (CDC and WorldHealth Organization), an epi-demiology and disease surveil-lance computer software pack-age. The frequency of accidentalexposures was assessed by- category ofworker (facultymember, resident, dental stu-dent, hygienist, dental assis-tant, staff member);- year of exposure;- location of injury (dental op-eratory, oral surgery, steriliza-tion area, dental laboratory, op-erating room, emergency room);
TABLE 'I
- mechanism of exposure tofinger or thumb, hand, face,arm, or foot or leg (syringe nee-dle, suture needle, bur, scalpelblade, wire, explorer, scaler orcurette, other instrument,splashes or bites);- action performed;- HIV status by self-report ofsource patient.
To assess the denominatordata for the calculation of expo-sures per patient visit, we de-termined the number of dentalvisits by reviewing computer-ized billing data at each studysite. Person-years of exposureeligibility for each occupationalcategory were estimated by in-terviewing administrativesources at each study site to es-timate the number of person-years spent in clinical activities.
Underreporting survey. Inconjunction with this study, wealso conducted a survey to esti-mate the extent to which the ac-cidental exposures among den-tal health care workers at thestudy sites were underreported.In 1995, 500 dental health careworkers at UCSF were asked toreport, on an anonymous survey
form, the number of accidentalblood exposures that they hadexperienced and the number ofexposures that they had report-ed during the last calendaryear. If a dental health careworker did not report an expo-sure, the respondent was askedto explain why he or she did notreport it.
RESULTS
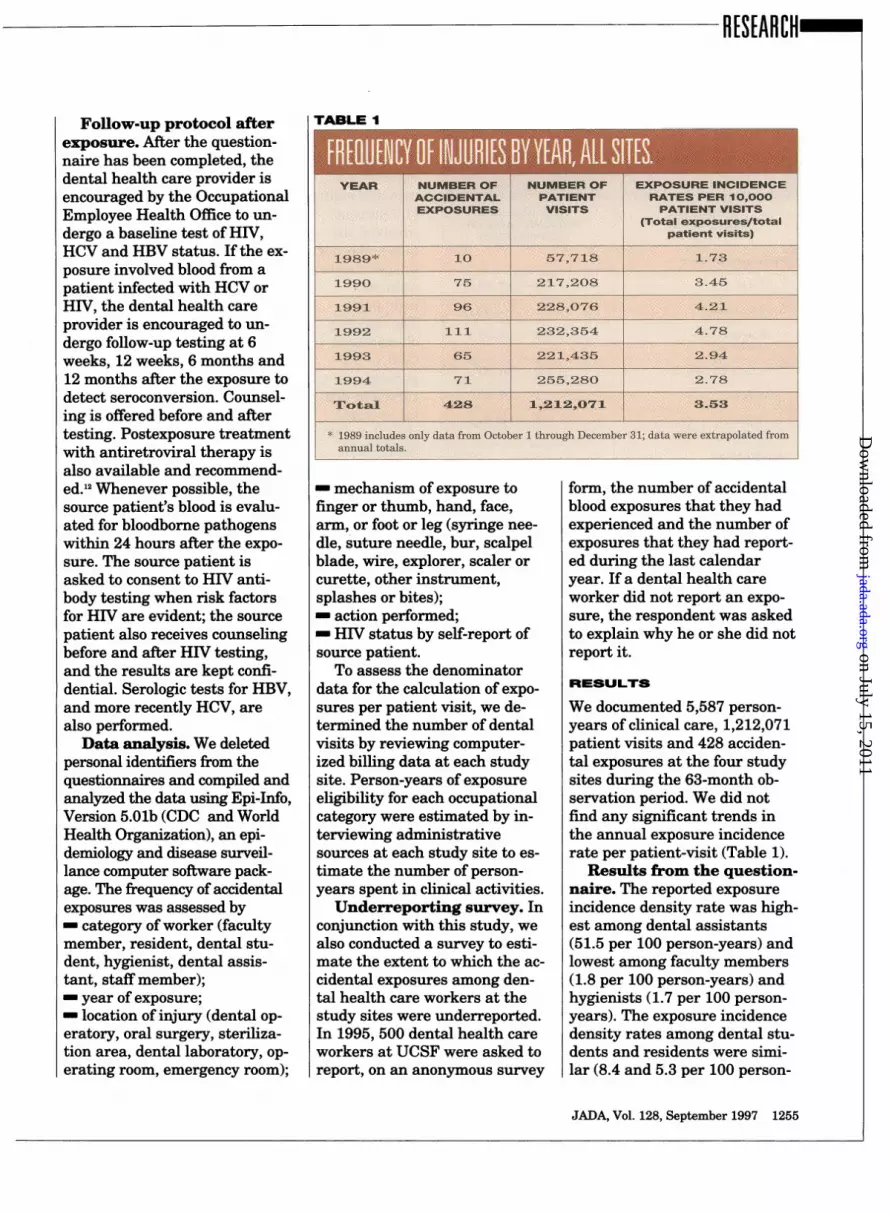
We documented 5,587 person-years of clinical care, 1,212,071patient visits and 428 acciden-tal exposures at the four studysites during the 63-month ob-servation period. We did notfind any significant trends inthe annual exposure incidencerate per patient-visit (Table 1).
Results from the question-naire. The reported exposureincidence density rate was high-est among dental assistants(51.5 per 100 person-years) andlowest among faculty members(1.8 per 100 person-years) andhygienists (1.7 per 100 person-years). The exposure incidencedensity rates among dental stu-dents and residents were simi-lar (8.4 and 5.3 per 100 person-
Total 428 (100*)* 8p1..h was t.fa. sass 31 QaO .as a.4&31W4.5 .tei.t.intwocsses.
years, respectively). There wereno significant epidemiologic dif-ferences in exposure incidencerates among the four studysites.
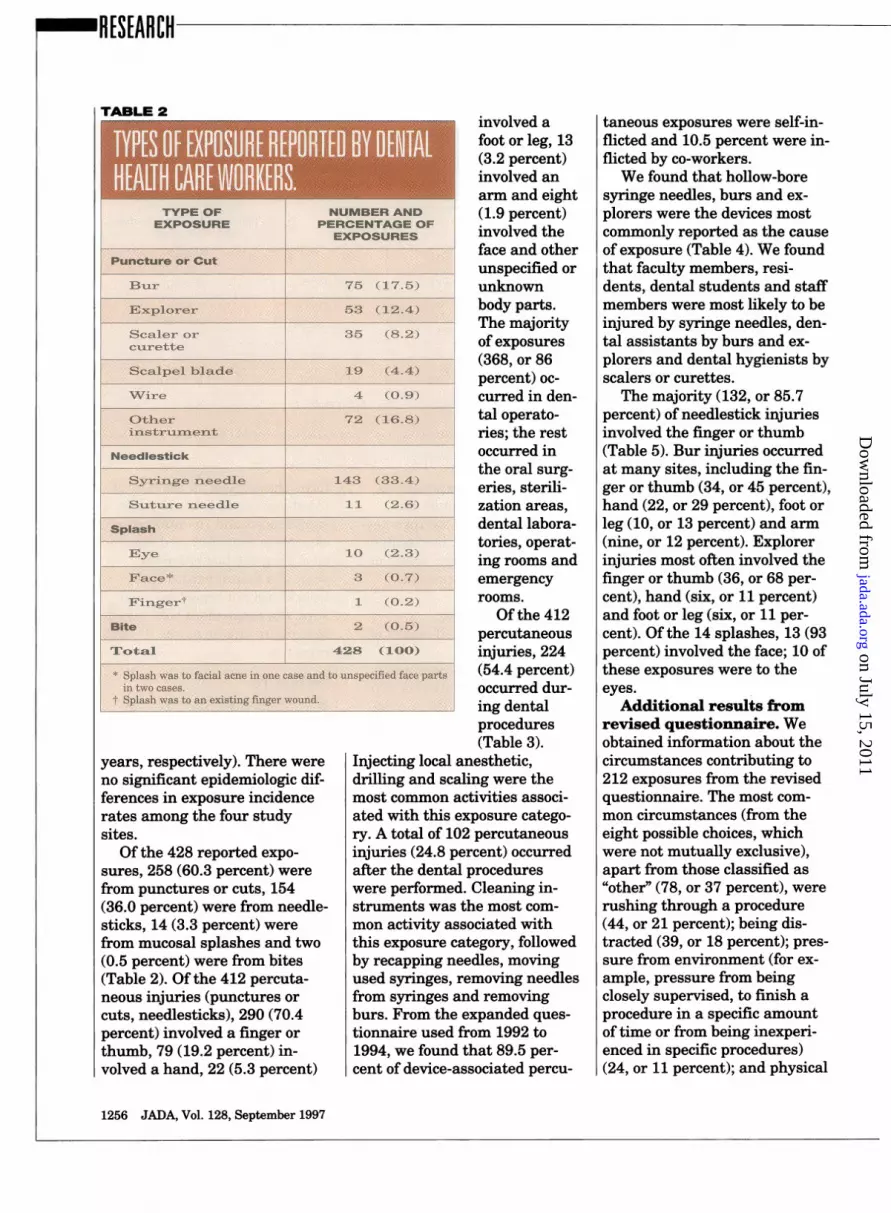
Of the 428 reported expo-sures, 258 (60.3 percent) werefrom punctures or cuts, 154(36.0 percent) were from needle-sticks, 14 (3.3 percent) werefrom mucosal splashes and two(0.5 percent) were from bites(Table 2). Of the 412 percuta-neous injuries (punctures orcuts, needlesticks), 290 (70.4percent) involved a finger orthumb, 79 (19.2 percent) in-volved a hand, 22 (5.3 percent)
involved afoot or leg, 13(3.2 percent)involved anarm and eight(1.9 percent)involved theface and otherunspecified orunknownbody parts.The majorityof exposures(368, or 86percent) oc-curred in den-tal operato-ries; the restoccurred inthe oral surg-eries, sterili-zation areas,dental labora-tories, operat-ing rooms andemergencyrooms.
Of the 412percutaneousinjuries, 224(54.4 percent)occurred dur-ing dentalprocedures(Table 3).
Injecting local anesthetic,drilling and scaling were themost common activities associ-ated with this exposure catego-ry. A total of 102 percutaneousinjuries (24.8 percent) occurredafter the dental procedureswere performed. Cleaning in-struments was the most com-mon activity associated withthis exposure category, followedby recapping needles, movingused syringes, removing needlesfrom syringes and removingburs. From the expanded ques-tionnaire used from 1992 to1994, we found that 89.5 per-cent of device-associated percu-
taneous exposures were self-in-flicted and 10.5 percent were in-flicted by co-workers.We found that hollow-bore
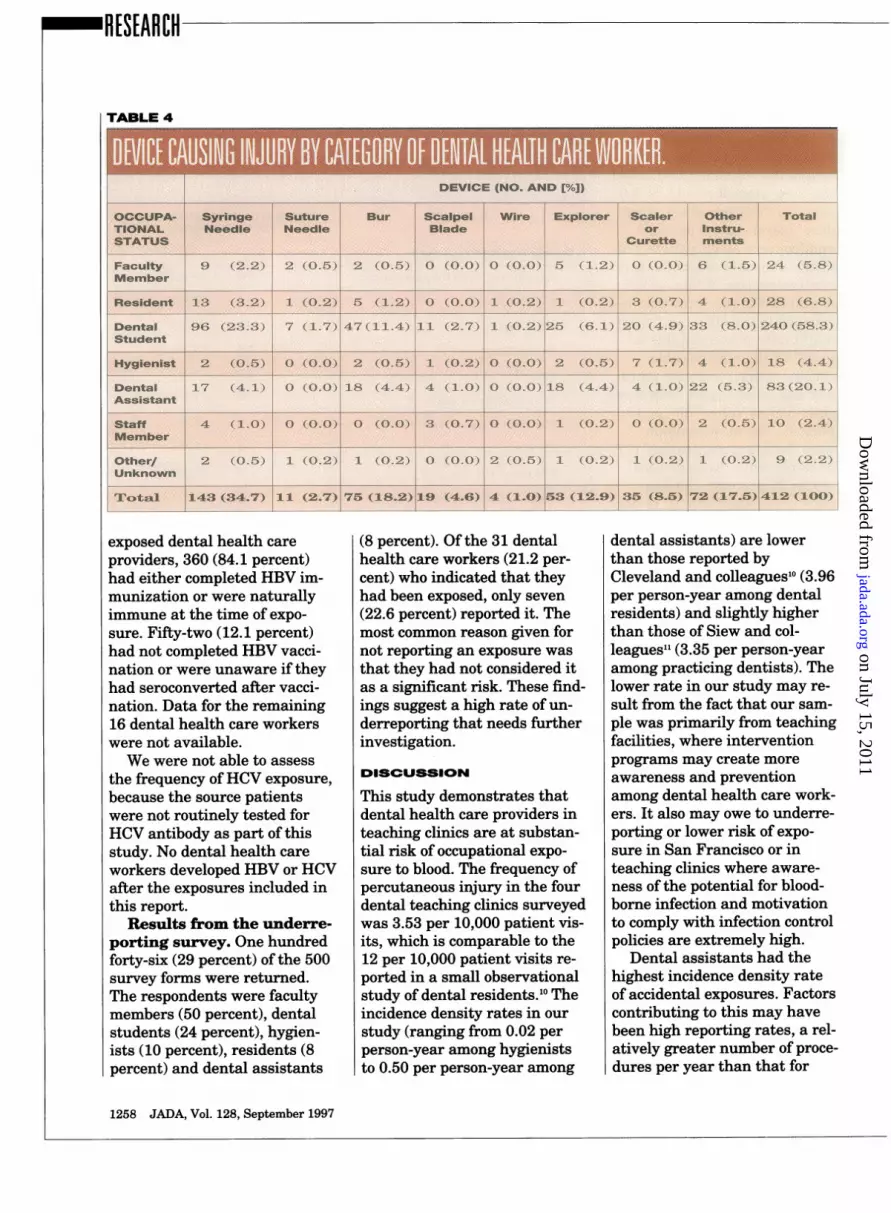
syringe needles, burs and ex-plorers were the devices mostcommonly reported as the causeof exposure (Table 4). We foundthat faculty members, resi-dents, dental students and staffmembers were most likely to beinjured by syringe needles, den-tal assistants by burs and ex-plorers and dental hygienists byscalers or curettes.
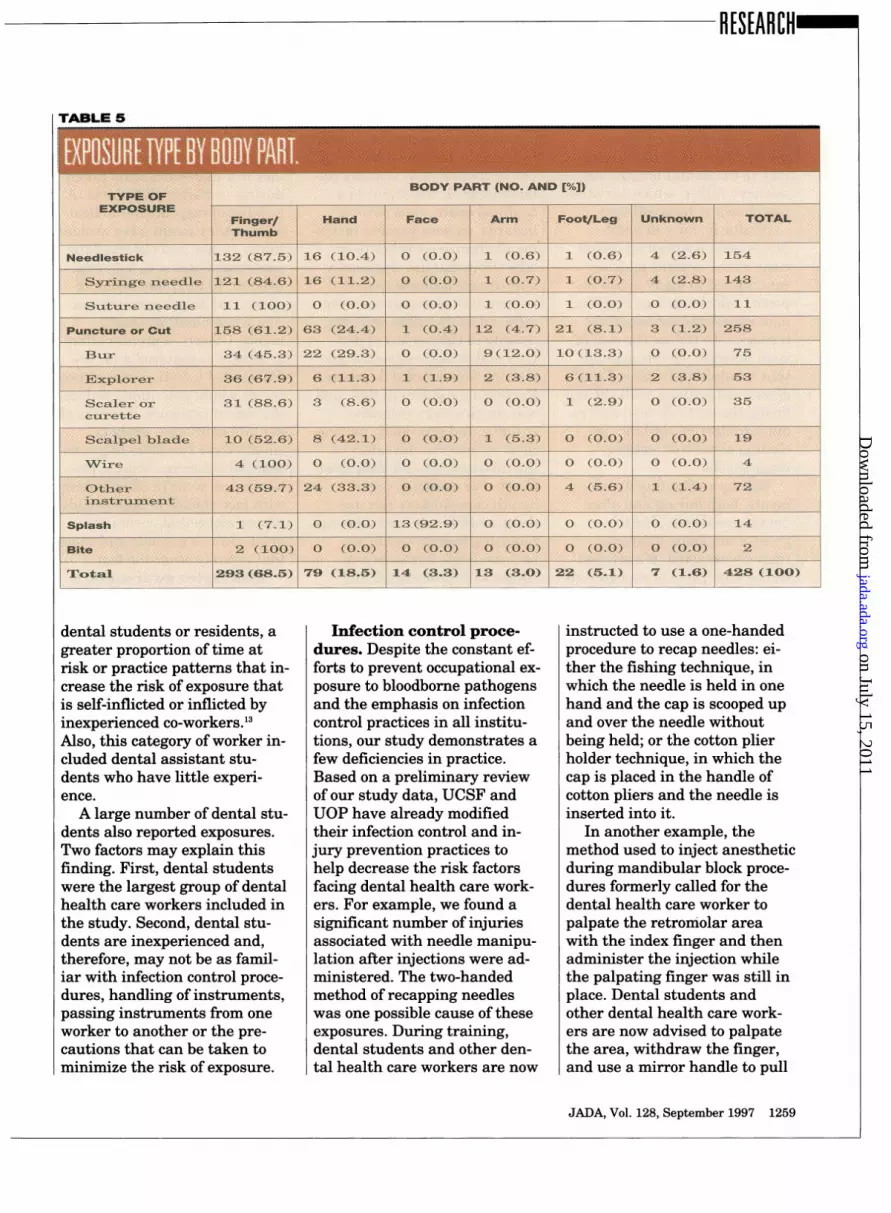
The majority (132, or 85.7percent) of needlestick injuriesinvolved the finger or thumb(Table 5). Bur injuries occurredat many sites, including the fin-ger or thumb (34, or 45 percent),hand (22, or 29 percent), foot orleg (10, or 13 percent) and arm(nine, or 12 percent). Explorerinjuries most often involved thefinger or thumb (36, or 68 per-cent), hand (six, or 11 percent)and foot or leg (six, or 11 per-cent). Of the 14 splashes, 13 (93percent) involved the face; 10 ofthese exposures were to theeyes.
Additional results fromrevised questionnaire. Weobtained information about thecircumstances contributing to212 exposures from the revisedquestionnaire. The most com-mon circumstances (from theeight possible choices, whichwere not mutually exclusive),apart from those classified as"other" (78, or 37 percent), wererushing through a procedure(44, or 21 percent); being dis-tracted (39, or 18 percent); pres-sure from environment (for ex-ample, pressure from beingclosely supervised, to finish aprocedure in a specific amountof time or from being inexperi-enced in specific procedures)(24, or 11 percent); and physical
location of the instrument trayin the dental operatory (21, or10 percent). Fewer than 5 per-cent of the respondents checkedthe "new procedure" (11, or 5.0percent), "concern about proce-dure" (seven, or 3.0 percent)and "concern about patient's in-fection/illness" (two, or 0.9 per-cent) categories. A total of 205dental health care providers re-sponded to the question, "Whatmight have prevented this in-jury?" Of the nine possiblechoices-which were not mutu-ally exclusive-apart from thoseclassified as "other" (30, or 15percent), the most commonwere "better concentration" (77,or 38 percent), "safer devices"(38, or 19 percent), "havingmore experience" (28, or 14 per-cent) and "less pressure" (27, or13 percent). "Better personalsafety equipment," "more assis-tance," "more time" and "moreinstruction" were each checkedby fewer than 10 percent of therespondents.
Based on all 428 reported ex-posures, gloves were the mostcommon protective barrier usedby the dental health care work-ers. However, they were notworn in 49 (11.4 percent) of thereported exposures. The dentalhealth care workers did notwear eye protection (glasses ora face shield) in 114 (26.6 per-cent) of exposures, face masksin 134 (31.3 percent) of the ex-posures or protective gowns in180 (42.1 percent) of exposures.
Superfi'cial scratches or punc-tures without bleeding made up378 (83 percent) of the 428 re-ported exposures. The 20 (5 per-cent) deep exposures in whichbleeding occurred were causedby syringe needles (six, or 30percent), scalpel blades (four, or20 percent), scalers or curettes(two, or 10 percent), burs (two,
TABLE 3
Irecig oclansteic7 (1.8.4)
ADril 52, (12.6)
Suturing 16~~~~~~~i (3.9)
Rteaching for insOtr*ument 13 (3.2)
Performing extractions ~4 (1.0)
Filing ~~~~~~~~~4(1.0)
Manipulatngwire 4 (1-0)
Per-formig ndodontic 3 (0.7)
trea,..tment
Cleaninginstruments ~~72 (17.5)
Moving use2syring
or 10 percent), explorers (one,or 5 percent), suture needles(one, or 5 percent) and other in-struments (four, or 20 percent).
In 286 (67 percent) of the 428exposures, the source patientsknew their HIV status at thetime the exposures were report-ed. Overall, 71 source patients(17 percent) were infected withHIV, and 40 of these patientsmet the criteria for havingAIDS. The characteristics of ex-posures involving blood frompatients with HIV did not differfrom those involving the 215 (50percent) noninfected patients
and the 142 (33 percent) pa-tients who did not know theirHIV status. Although many ofthe exposures to HIV-contami-nated blood were inflicted bysharp instruments, none of the71 dental care providers whowere exposed to blood and bodyfluids from patients with HIVbecame infected.
In addition, 18 (4.2 percent)source patients were infectedwith HBV; 243 (56.8 percent)source patients were not infect-ed with HBV and the status of167 (39.0 percent) source pa-tients was unknown. Of the 428
exposed dental health careproviders, 360 (84.1 percent)had either completed HBV im-munization or were naturallyimmune at the time of expo-sure. Fifty-two (12.1 percent)had not completed HBV vacci-nation or were unaware if theyhad seroconverted after vacci-nation. Data for the remaining16 dental health care workerswere not available.We were not able to assess
the frequency ofHCV exposure,because the source patientswere not routinely tested forHCV antibody as part of thisstudy. No dental health careworkers developed HBV or HCVafter the exposures included inthis report.
Results from the underre-porting survey. One hundredforty-six (29 percent) of the 500survey forms were returned.The respondents were facultymembers (50 percent), dentalstudents (24 percent), hygien-ists (10 percent), residents (8percent) and dental assistants
(8 percent). Ofthe 31 dentalhealth care workers (21.2 per-cent) who indicated that theyhad been exposed, only seven(22.6 percent) reported it. Themost common reason given fornot reporting an exposure wasthat they had not considered itas a significant risk. These find-ings suggest a high rate of un-derreporting that needs furtherinvestigation.
DISCUSSION
This study demonstrates thatdental health care providers inteaching clinics are at substan-tial risk of occupational expo-sure to blood. The frequency ofpercutaneous injury in the fourdental teaching clinics surveyedwas 3.53 per 10,000 patient vis-its, which is comparable to the12 per 10,000 patient visits re-ported in a small observationalstudy of dental residents.10 Theincidence density rates in ourstudy (ranging from 0.02 perperson-year among hygieniststo 0.50 per person-year among
dental assistants) are lowerthan those reported byCleveland and colleagues'o (3.96per person-year among dentalresidents) and slightly higherthan those of Siew and col-leagues"l (3.35 per person-yearamong practicing dentists). Thelower rate in our study may re-sult from the fact that our sam-ple was primarily from teachingfacilities, where interventionprograms may create moreawareness and preventionamong dental health care work-ers. It also may owe to underre-porting or lower risk of expo-sure in San Francisco or inteaching clinics where aware-ness of the potential for blood-borne infection and motivationto comply with infection controlpolicies are extremely high.
Dental assistants had thehighest incidence density rateof accidental exposures. Factorscontributing to this may havebeen high reporting rates, a rel-atively greater number of proce-dures per year than that for
dental students or residents, agreater proportion of time atrisk or practice patterns that in-crease the risk of exposure thatis self-inflicted or inflicted byinexperienced co-workers.'3Also, this category of worker in-cluded dental assistant stu-dents who have little experi-ence.A large number of dental stu-
dents also reported exposures.Two factors may explain thisfinding. First, dental studentswere the largest group of dentalhealth care workers included inthe study. Second, dental stu-dents are inexperienced and,therefore, may not be as famil-iar with infection control proce-dures, handling of instruments,passing instruments from oneworker to another or the pre-cautions that can be taken tominimize the risk of exposure.
Infection control proce-dures. Despite the constant ef-forts to prevent occupational ex-posure to bloodborne pathogensand the emphasis on infectioncontrol practices -in all institu-tions, our study demonstrates afew deficiencies in practice.Based on a preliminary reviewof our study data, UCSF andUOP have already modifiedtheir infection control and in-jury prevention practices tohelp decrease the risk factorsfacing dental health care work-ers. For example, we found asignificant number of injuriesassociated with needle manipu-lation after injections were ad-ministered. The two-handedmethod of recapping needleswas one possible cause of theseexposures. During training,dental students and other den-tal health care workers are now
instructed to use a one-handedprocedure to recap needles: ei-ther the fishing technique, inwhich the needle is held in onehand and the cap is scooped upand over the needle withoutbeing held; or the cotton plierholder technique, in which thecap is placed in the handle ofcotton pliers and the needle isinserted into it.
In another example, themethod used to inject anestheticduring mandibular block proce-dures formerly called for thedental health care worker topalpate the retromolar areawith the index finger and thenadminister the injection whilethe palpating finger was still inplace. Dental students andother dental health care work-ers are now advised to palpatethe area, withdraw the finger,and use a mirror handle to pull
aside the cheek while the injec-tion is administered. Thismethod reduces the risk of in-jury to the dental health careworker's finger, which our studyhas shown to be significant.
Similarly, burs in hand-pieces, which rested on dentalcarts in the upright position,contributed to many of the re-ported injuries to legs and feetand, in several instances, thebuttocks. To reduce the risk ofsuch injuries, we recommendthat handpieces be placed in thedownward position with the burfacing the cart. We also now re-quire protective clothing, in-cluding shoes that entirelycover the feet.
Wiping or cleaning instru-ments, both during and afterdental procedures, led togreater numbers of injuriesthan we expected. We attribut-ed the high rates of exposure re-ported in our study to the elabo-rate cleaning process, whichinvolved many stages and re-peated handling of the instru-ments. These findings promptedus to revise the cleaning pro-cess. Instrument handling isnow minimized, and the num-ber of steps involved has beenreduced. Dental health careworkers are encouraged to weartwo layers of gloves when clean-ing instruments: examinationgloves next to the skin, coveredby heavy-duty, or utility, outerrubber gloves. Cleaning instru-ments during dental procedures(for example, wiping of instru-ments with gauze and thecleaning burs) might also causeaccidental exposures, but ourdata regarding these proceduresare not conclusive.
Nonetheless, the greatest riskis posed by accidental exposuresduring dental procedures wheninstruments are used for their
intended purpose. Intraoral in-strument manipulation-eitherby a single dental worker or bytwo or more dental workers col-laborating on treatment in aconfined space-has obvioushazards, as does passing instru-ments from one worker to an-other (four-handed dentistry).Our results indicate that 10.5percent (23) of exposures wereinflicted by dental co-workers,usually in the context of den-tists and dental assistants per-forming four-handed dentistry.Preventing injuries in this areawill require more extensivetraining and ergonomic innova-tions to improve the safety ofthe instruments and their easeof use. For example, dentalhealth care workers can usemore consistently instrumentsrequiring less manipulation,such as single-use safety sy-ringes with preinserted andnonremovable needles. More-over, both dentists and their as-sistants should receive additionaleducation in four-handed den-tistry, as part of their training.
Even though our study didnot specifically assess the riskof handling materials in dentallaboratories, we did observesome injuries. It is possible thatinfectious material in laboratoryelements, such as dental im-pressions, might be a source ofexposure. The risks of injury insuch contexts require furtherstudy.
Risk of exposure precau-tions. The most frequentlycited circumstances contribut-ing to injury were being dis-tracted (39, 18 percent) andrushing through the procedure(44, 21 percent). These findingssuggest that dental health careworkers need to pay greater at-tention to the mental aspects ofprocedures to avoid injury and
minimize exposures.Another potential cause of
the reported exposures was thelack of sufficient caution takenduring and after procedures. Anumber of respondents indicat-ed that they might have avoidedinjury if they had observed therecommendations to not recapneedles, to wear two layers ofgloves and to use extreme cau-tion when handling instru-ments. Clearly, a greater effortto adhere to required and rec-ommended infection control pro-cesses would potentially reducethe risk of exposure. Perhaps alldental health care workersshould wear two pairs of glovesespecially during cleanup, pro-tective eye wear in combinationwith face shields or side shields,proper attire that covers asmuch skin as possible and shoesthat entirely cover the feet.
Risk factor awareness. Itis possible that some workersare not completely aware of theadditional risk factors accompa-nying certain procedures or ofthe comparatively significantrisk of HCV. It should be a highpriority that all dental healthcare workers are educatedabout bloodborne pathogentransmission in all possible set-tings and about all recommend-ed preventive measures.However, it should be under-stood that the ultimate respon-sibility lies with individual den-tal health care workers tocomply and adopt appropriatepreventive practices.
Despite the existence of aneffective vaccine, 52 (12.8 per-cent) of the dental health careworkers reporting exposureswere susceptible to infection byHBV. This finding indicatesthat there is still reluctance onthe part of some dental healthcare workers to be vaccinated or
sor, Division of orali medicine,peiatr Dentlsti Department of
Department of Stomatology and
Growth and Develop. Oral AIDS Center,ment, and member University of
of the Oral AIDS California, SanCenter, Departmient Francisco.
of Stomatology,University of
Caom la, San
Calforia.San complete a vac-Fr-ancIsco, 707
Ave. cination series,D.Rmoom zD 1Box and it shows a
0438, San Francisco,Caif "'10 4 need to encour-Address reprintof age and rein-uests to Dr.Riforce-and per-
haps require-dental health care workers tocomplete vaccination require-ments before beginning clinicalwork. The feasibility of imple-menting more efficient and com-prehensive mechanisms to mon-itor worker vaccinations shouldbe examined, as some workerswere not aware that seroconver-sion had not occurred, evenafter completing the requiredthree vaccinations.
At the time this study tookplace, the only available recom-mended therapy for exposedpeople was antiretroviral thera-py (mainly azidothymidine).Today, the exposed dentalhealth care worker has accessto multidrug therapies such asantiretroviral agents in combi-nation with protease inhibitors.In fact, such multidrug thera-pies have been highly recom-mended as a new postexposureprotocol. 12
Underreporting. One im-portant limitation of our studywas its reliance on self-report-ing of exposures. The needle-stick hotline was designed tominimize time delays and other
barriers to reporting and to in-crease incentives to report byproviding immediate expertconsultation. The response rateto our underreporting surveywas not sufficient to make anaccurate estimate of the truenumber of eligible exposures.However, among the 146 surveyrespondents, 31 indicated thatthey had had an accidental in-jury, yet 24 (77 percent) did notreport their exposures. Themajor reason cited for not re-porting was the belief that theexposure did not impart a sig-nificant risk of infection trans-mission.
CONCLUSION
Despite their limitations, thedata from this study representan attempt to establish someunderstanding of the extent ofunderreporting and to raiseawareness that this importantissue needs further investiga-tion. Efforts are under way toremind dental health careworkers about the ubiquitousnature of bloodborne pathogens,the inaccuracies inherent in re-lying on clinical criteria alone toassess the probability of infec-tion and the growing risk ofHCV infections in our patientpopulation. Further investiga-tion to better our understandingof factors that mitigate againstreporting-for example, thestigma associated with acciden-tal injury and the inconvenienceof reporting-and interventionsto encourage reporting are obvi-ously needed. o
Dr. Ellison is an assistant clinical professor,Department of Restorative Dentistry,University of California, San Francisco.
Dr. Bird is an associate clinical professor,Department of Restorative Dentistry,University of California, San Francisco.
Ms. Lowe is the former director of surgicalservices, Department of Oral Surgery,University of the Pacific, San Francisco.
Dr. Gerberding is an associate professor ofmedicine and epidemiology, Department ofEpidemiology and Prevention InterventionsCenter, San Francisco General Hospital andUniversity of California, San Francisco.
This research was supported by Macy'sWest Passport AIDS Benefit-UCSF Fund.
The research in this article was presented asa poster at the 74th General Session of theInternational Association for Dental Research,San Francisco, March 1996.
The authors are grateful to Dr. John C.Greene; Dr. Peter L. Jacobsen; the Universityof California, San Francisco exposure hotlinecoordinator, Ms. Ellie Lannen; and the SanFrancisco General Hospital/Epi-Center stafffor their support in the development of thestudy. They are also grateful to StephenOrdway and Evangeline Leash for their edito-rial contributions.
1. Bell DM. Human immunodeficiency virustransmission in health care settings: risk andrisk reduction. Am J Med 1991;91(3B):294S-300S.
2. Verrusio AC. Risk of transmission of thehuman immunodeficiency virus to health careworkers exposed to HIV-infected patients: areview. JADA 1989;118:339-42.
3. Gerberding JL. Management of occupa-tional exposures to blood-borne viruses. NEngl J Med 1995;332(7):444-51.
4. Henderson DK, Fahey BJ, Willy M, et al.Risk for occupational transmission of humanimmunodeficiency virus type 1 (HIV-1) associ-ated with clinical exposures: a prospectiveevaluation. Ann Intern Med 1990;113:740-6.
5. Ippolito G, Puro V, DeCarli G. The risk ofoccupational human immunodeficiency virusinfection in health-care workers: Italian multi-center study. Arch Intern Med 1993;153:451-8.
6. Tokars JI, Marcus R, Culver DH, et al.Surveillance ofHIV infection and zidovudineuse among health-care workers after occupa-tional exposure to HIV-infected blood. AnnIntern Med 1993;118(12):913-9.
7. Kein RS, Phelan JA, Freeman K, et al.Low occupational risk of human immunodefi-ciency virus infection among dental profes-sionals. N Engl J Med 1988;318(2):86-90.
8. Capilouto EI, Weinstein MC, HemenwayD, Cotton D. What is the dentist's occupation-al risk ofbecoming infected with hepatitis Bor the human immunodeficiency virus? Am JPublic Health 1992;82:587-9.
9. Gooch BF, Cardo DM, Marcus R, et al.Percutaneous exposures to HIV-infected bloodamong dental workers enrolled in the CDCneedlestick study. JADA 1995;126(9):1237-42.
10. Cleveland JL, Lockwood SA, Gooch BF, etal. Percutaneous injuries in dentistry: an ob-servational study. JADA 1995;126(6):745-51.
11. Siew C, Gruninger SE, Miaw CL, NeidleEA. Percutaneous injuries in practicing den-tists: a prospective study using a 20-daydiary. JADA 1995;126:1227-34.
12. Gerberding JL. Prophylaxis for occupa-tional exposure to HIV. Ann Intern Med1996;125(6):497-501.